

Introduction:
Paroxysmal cold hemoglobinuria (PCH) is a rare autoimmune hemolytic anemia (AIHA) that causes intravascular hemolysis and profound, sometimes life-threatening anemia. It most commonly occurs in children following viral infection, and presents with acute onset anemia, pallor, jaundice, and hemoglobinuria. PCH is caused by a biphasic immunoglobulin G (IgG) autoantibody that targets the P-antigen on red blood cells (RBCs) with complement fixation at low temperatures. Subsequent warming in the central circulation leads to complement activation and intravascular hemolysis. Management of PCH has been primarily supportive, with environmental warming to prevent autoantibody binding and transfusion with warmed packed red blood cells (PRBCs) as clinically indicated. Efficacy of corticosteroids has not been demonstrated. We report on successful treatment of PCH by complement blockade using a single dose of eculizumab.
Case Description:
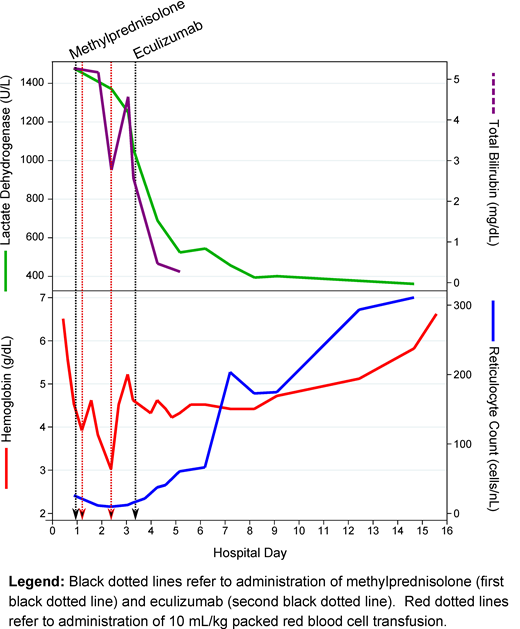
We treated a previously healthy 4-year-old boy who presented with 5-day history of transient maculopapular rash, 3-day history of fatigue, thigh and abdominal pain, 2-day history of cough, chills, vomiting, diarrhea and high-grade fevers, and on the day of presentation, developed jaundice and dark urine. Hemoglobin (Hgb) level was 6.4 g/dL at a primary care visit. On admission, he was febrile, tachycardic, with scleral icterus and pallor, worsening anemia (Hgb 5.6 g/dL) which 1 hour later dropped to 4.5 g/dL, with reticulocytopenia, spherocytosis, and positive direct antiglobulin test (DAT). Initially he received methylprednisolone as empiric treatment for AIHA. Monospecific DAT was positive for C3d and negative for IgG, leading to suspicion of cold-antibody mediated AIHA (cAIHA). Due to hemoglobinuria consistent with intravascular hemolysis, PCH was suspected and a Donath-Landsteiner (DL) test was ordered. Despite environmental warming and azithromycin for potential Mycoplasma pneumoniae induced cold agglutinin syndrome, he developed worsening anemia (nadir Hgb 3.0 g/dL) with signs of shock including altered mental status, tachycardia, lactic acidosis, and high oxygen extraction, and continued transfusion requirement. On hospital day 4, we decided to treat him with eculizumab 600 mg intravenously. That afternoon, definitive testing for PCH with the DL test returned positive, confirming PCH diagnosis. Markers of hemolysis, including lactate dehydrogenase and bilirubin, decreased immediately following eculizumab administration. No further transfusion was required. Hgb levels stabilized, and reticulocyte counts increased daily. Steroids were discontinued on hospital day 6. Complete complement blockade following a single dose of eculizumab was confirmed on hospital day 7, with total complement level (CH50) reported as <13.8 U/mL. The patient continued to improve and was discharged home on hospital day 15 with Hgb 6.6 g/dL, improving to 9.1 g/dL 6 days later. Diagnostic tests for infectious and toxin-mediated causes of PCH remained negative. He was given prophylaxis for encapsulated bacterial infections with penicillin VK, given increased risk of infection from ongoing complement blockade and his unvaccinated status. This was discontinued when CH50 levels normalized, 42 days after eculizumab administration.
Discussion:
To our knowledge, this is the first published observation of successful complement blockade for the treatment of PCH. Complement is a key effector of intravascular hemolysis in PCH. Eculizumab, an anti-C5 monoclonal antibody that blocks the terminal complement pathway, resulted in an efficient, complete, and sustained clinical improvement following a single dose. We observed no adverse effects. This case suggests a need for further investigation of complement-blockade, either at the terminal pathway or classical pathway level, in the treatment of this disease.
Berentsen:Apellis: Consultancy, Honoraria; Alexion: Honoraria; Bioverativ, a Sanofi company: Consultancy, Honoraria; Janssen-Cilag: Honoraria; Mundipharma: Research Funding; True North Therapeutics: Consultancy, Honoraria.
Eculizumab for paroxysmal cold hemoglobinuria

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal