

Objective: To describe the characteristics and outcomes of chronic myeloid leukemia (CML) patients treated through the Glivec Patient Assistance Program (GIPAP) in Rwanda.
Methods: We retrospectively reviewed all BCR-ABL positive CML patients treated with imatinib at two rural hospitals between 2009 and 2018. Clinical data were analyzed using descriptive statistics, Kaplan-Meier method, and proportional hazards regression.
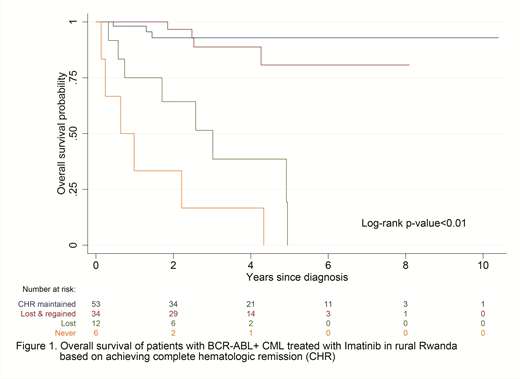
Results: One hundred twenty-four patients were included; median age 35 (range: 9-81), 60% male, 88% without comorbidities. All patients presented with symptomatic disease, median duration 11 months (IQR: 4-24) and median WBC count 225.5 x 109/L (IQR: 117.7-308.5). At diagnosis, 71% were in chronic phase. On imatinib, 91% achieved complete hematologic remission (CHR); 67% within 90 days. Of those who achieved CHR, 51 (45%) lost it at some point and, of which, 36 (71%) regained CHR. At four years, overall survival was 79% (95% CI:69%-86%) for the entire cohort; 93% (95% CI: 79%-98%) for 53 patients who remained in CHR, 89% (95% CI: 69%-96%) for 34 patients who lost but regained CHR, 19% (95% CI: 1%-54%) for 12 patients who lost and never regained CHR. Never achieving CHR was associated with increased mortality (HR: 40.89; 95% CI: 9.88-169.32; p<0.001) as was losing CHR without regaining it (HR 15.73; 95% CI: 4.14-59.81; p<0.001) compared to never losing CHR.
Conclusions: Here we demonstrate the feasibility of coupling molecular diagnostics with chronic targeted therapy in a rural low-resource setting through health systems strengthening and international collaboration. Our CML patients are younger, slower to achieve CHR with imatinib, and have higher rates of primary and early hematologic resistance than historical cohorts, suggesting biological differences that warrant further investigation. It is uncertain what role non-adherence to medication influences these data. Without molecular response assessment, hematologic response is an accurate marker of disease control and survival. Our imatinib failure rates highlight the need for access to resistance testing and second generation tyrosine kinase inhibitors, as well as adherence rates.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal