

Introduction
Due to recent changes in acute leukemia treatment, there is an urgent need for greater understanding of the factors affecting quality of life at different points in the journey of patients. The Acute Leukemia Advocates Network (ALAN) is running a multi-country survey to gather information on the experiences, quality of life and symptoms of adults (16+) with different types of acute leukemia.
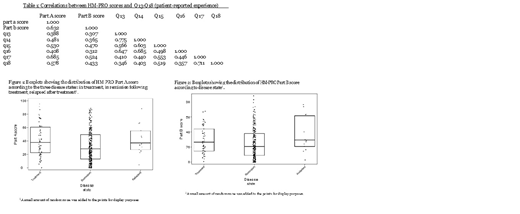
The study objectives were to: (1) investigate whether the HM-PRO scores differ according to disease state; (2) determine whether those with worse scores on Q13-Q18 (patient-reported experience) will also report higher HM-PRO scores (a worse quality of life); (3) examine if there are significant differences for the HM-PRO scores between acute leukemia types and gender.
Methods
This survey comprises 99 items and was designed based on a literature review of quality of life and acute leukemia followed by input from clinical and patient advocacy experts. HM-PRO, an instrument to measure patient-reported outcomes in patients with hematological malignancies, was incorporated into the survey for assessing quality of life and symptoms. This is a composite measure consisting of: Part A (impact/quality of life); and Part B (signs and symptoms). A higher score in each part represents more impaired outcomes.
Question 9 provides a measure for disease state (undergoing treatment, in remission following treatment or relapsed following treatment).
We hypothesised that patients with a worse experience in each of the following areas would report a worse overall quality of life: physical symptoms and side effects (Q13), emotional impact (Q14), physical and mental health (Q15), information from healthcare professionals (Q16), ability to perform meaningful activities (Q17) and well-being of carers, friends and family (Q18). These are itemised on an interval scale ranging from 0-10, where 0 represents a bad experience and 10, a good experience.
Questions 19-99 investigated further each of the hypotheses, to identify patient issues and background demographic questions. The survey was translated into 9 languages and promoted via patient advocacy groups from 1/3/19 to 31/5/19 (ongoing).
Spearman correlation analysis was used to determine the direction and strength of relationships between the measures. Two sample Wilcoxon rank-sum tests and Kruskal-Wallis rank test were applied to test for differences between groups.
Results
There were 371 respondents: acute myeloid leukemia (213), acute lymphoblastic leukemia (86) and acute promyelocytic leukemia (72). There was no evidence of any difference in the HM-PRO score for either Part A - quality of life (p=0.9) or Part B - signs and symptoms (p=0.4) between acute leukemia types.
Of these 149 were men and 219 female and 3 provided no gender. The median Part A score for males and females was 24.1 and 30.39, respectively (p=0.07). The median for Part B was 17.6 and 23.5 for males and females, respectively (p=0.01) with females reporting greater burden of signs and symptoms.
The analysis suggests that there is a difference in the HM-PRO scores between disease state, with those in remission following treatment having lower HM-PRO scores (better quality of life) than those currently undergoing treatment (Figure 1&2).
The results confirmed our hypotheses that those with worse scores for Q13-Q18 have a worse quality of life (higher HM-PRO score). The responses to all of these questions were either weakly or moderately related to scores of both parts of the HM-PRO (Table 1). The correlations (negative) were all statistically significant, suggesting that low HM-PRO scores are associated with good experiences and vice versa. Some individual questions were also highly correlated (rs = ≥0.7) with one another (e.g. Q14 and Q13, or Q17 and Q18), showing internal stability of the items.
Conclusion
The study confirms that acute leukemia patients in remission report a better quality of life than those currently undergoing treatment. However, there is no evidence of any difference in the HM-PRO scores between acute leukemia types which needs to be further explored in controlled studies. In terms of gender differences, the results indicate that female patients experience greater impact on quality of life and symptoms. Furthermore, patients with worse reported experience (Q13-18) have a lower overall quality of life, suggesting that improving support in these areas may enhance overall quality of life.
Pemberton-Whiteley:CML Advocates Network: Membership on an entity's Board of Directors or advisory committees; Patient Evidence: Equity Ownership; AbbVie: Other: Grant funding; Amgen: Consultancy, Other: Grant funding, Speakers Bureau; Bristol-Myers Squibb: Consultancy, Other: Grant funding, Speakers Bureau; Celgene: Consultancy, Other: Grant funding; Acute Leukemia Advocates Network (ALAN): Consultancy; Pfizer: Consultancy, Other: Grant Funding, Speakers Bureau; Takeda: Other: Grant funding; Shire: Other: Grant Funding; Kyowa Kirin: Other: Grant funding; Novartis: Consultancy, Other: Grant funding, Speakers Bureau; Incyte: Consultancy, Other: Grant funding; Jazz: Other: Grant funding, Speakers Bureau; Janssen: Consultancy, Other: Grant funding; Daiichi Sankyo: Other: Grant funding; Gilead: Other: Grant funding, Speakers Bureau; Leukaemia Care: Employment. Oliva:Celgene Corporation: Consultancy, Honoraria, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Apellis: Consultancy. Geissler:Incyte: Research Funding; Roche: Consultancy; Novartis: Consultancy, Research Funding, Speakers Bureau; Janssen: Consultancy, Speakers Bureau; UCB: Consultancy, Speakers Bureau; Servier: Consultancy; Takeda: Research Funding; Pfizer: Consultancy, Research Funding, Speakers Bureau; Biomarin: Consultancy; Amgen: Consultancy; Bristol-Myers Squibb: Consultancy, Research Funding, Speakers Bureau. Wintrich:Takeda: Consultancy; Janssen: Other: Grant Funding; Celgene: Other: Grant Funding; Novartis: Consultancy, Other: Grant Funding. Salek:Pfizer: Honoraria, Speakers Bureau; Merck: Consultancy; Agios Pharmaceuticals, Inc.: Consultancy, Honoraria. Ionova:Takeda, BMS: Other: Principal Investigator of IISR, Research Funding. Tate:Quality Health: Employment. Bradley:Quality Health: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal