

Background: High morbidity and mortality in patient receiving hematopoietic Stem Cell Transplantation (HSCT) are resulted from lung complications. Diagnosis of the etiology affects the choice of treatment. The bronchoalveolar lavage (BAL) analysis is safe and widely accepted, which provide valuable information for pathogen identification in pulmonary infections diagnosis.
Aims: The aim of this study was to evaluate the diagnostic yield of multiple diagnostic methods in BAL fluid (BALF) microbiological analysis from HSCT patients, and determine clinically relevant cutoffs of (1→3)-β-D-glucan (BDG) level and CMV virus load(VL) for pneumonia diagnosis.
Methods: This retrospective study enrolled 104 patients with pulmonary infiltrate between January 2016 and June 2019 at the Department of Hematology of the Shanghai General hospital(Table 1). This study was approved by the ethics committee of the Shanghai general hospital Institute. BAL sampling was routinely performed by trained physicians by fiberoptic bronchoscope. BALF samples were analyzed by microbiological culture, flow cytometry, PCR and mNGS.Data were analyzed by the Statistical Package of SPSS version 15.0 (SPSS, Inc., Chicago, IL, USA) for statistical analyses.Continuous variables were compared with Student's t-test.ROC curves were constructed to assess BDG for Pneumocystis jirovecii pneumonia (PJP),CMVDNA and the percent of CD4+T lymphocyte for CMV pneumonia
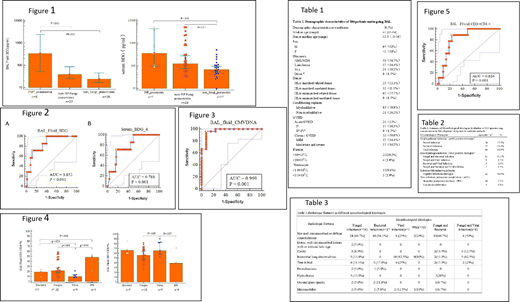
Results: All cases were examined by diverse methodology, including microbiological, radiologic, molecular and cytological methods. A total of 130 episodes of lung complication were identified in 104 patients. A specific diagnosis was obtained in 108 of the 130 episodes evaluated (83%)(Table 2).By microbiological method, The percentage of bacteria cultured from BALF was 19.2%, which was similar with that from sputum(17.7%).BALF culture produced better diagnostic yield of fungi than sputum (18.5% VS 8.5%, P=.028).In 95 episodes receiving GM test, 5 episodes were diagnosed as probable IA and 41 episodes as possible IA.At a cutoff optical density index (ODI) value of ≥0.7, the sensitivity of BALF GM detection was much higher than that of serum GM detection (71.7% versus 21.7%; P=0.001), but there was no significant difference between their specificities (91.8% versus 100%; P=0.68). BDG level were highest in patient with PJP than other fungi and non-fungi pneumonia(Figure 1).For the detection of suspected PJP, the sensitivity, specificity, the cutoff (pg/mL) of BDG was 71.43%, 88.89% and 161.2pg/ml in BAL fluid and 71.43%, 83.33% and 317.4pg/ml in serum(Figure 2). Radiologic results show that not well circumscribed or diffuse consolidations were common seen in bacterial infection(66.7%) and fungul infection(94.1%) and mixed infection(>50%), while interstitial lung abnormalities were seen in viral infection (62.5%) and IPS (90%) and mixed fungal and viral infection(62.5%)(Table 3). As target test of molecular diagnostic method, PCR analysis of BALF produced better diagnosis yield than serum and the sensitivity, specificity, CMVDNA cutoff (pg/mL) of PCR in BAL fluid was 96.3%, 92.31% and 8610 copy/ml(Figure 3). As unbias molecular diagnositic method, metagenomics (mNGS) results from 42 patients show positive agreement of 28.6% (12/42) and unique respiratory pathogens found of 14.3% (6/42) when compared with traditional culture and PCR testing method. In 28.6% (12/42) cases, the results of mNGS agreed with traditional culture and PCR, while pathogens were only detected by mNGS in 6 cases (14.3% ) . The false negative rate of mNGS was 22.2%, and the specificity was 54.5%. Flow cytometry results show that CD4+/CD8+ T cells in BALF were significantly different between infectious disease and idiopathic pneumonia. CD4+ T cells in BALF were lowest in CMV pneumonia when compared with bacteria and fungi infection and IPS(Figure 4). For the detection of suspected CMV pneumonia, the sensitivity, specificity and percentage cutoff of CD4+T cells in BALF were 88.89%, 80.49% and 13.74%(Figure 5).
Conclusion: Each method applied in this study shows unique advantage in diagnosis of lung complication following HSCT with BAL based analysis. mNGS cannot replace either culture or PCR, but it is useful in culture-negative patients. Combination of multiple examination is required. Cytology analysis and flow cytometry of BALF facilitated the etiology diagnosis in HSCT patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal