

[Introduction]
Transplant-associated thrombotic microangiopathy (TA-TMA) is a fatal complication after allogeneic hematopoietic stem cell transplantation (HSCT). However, given its relatively low incidence, no large cohort-based study has determined TA-TMA risk factors and its impact on overall survival (OS) or the most effective therapeutic interventions. Recombinant human soluble thrombomodulin (rTM) is a promising therapeutic option; with dual antithrombosis and anti-inflammation activities, a single-center small cohort study in Japan reported rTM to be effective against TA-TMA. This study aimed to clarify risk factors for TA-TMA development and the efficacy of various TA-TMA therapies in a multicenter large cohort.
[Methods]
This retrospective cohort study conducted by the Kyoto Stem Cell Transplantation Group enrolled adult patients (age ≥ 16 years) with hematological diseases who underwent allogenic HSCT after 2000. Cumulative TA-TMA incidence was calculated using Gray's test; death from any cause was a competing risk. We evaluated OS in patients with or without TA-TMA using the Simon-Makuch method and compared it using the Cox proportional hazard model with TA-TMA development as a time-dependent covariate. Correlations were analyzed between each pre- or post-transplant factor and TA-TMA development using Gray's test. Factors significant in the univariate analysis were subjected to the multivariate analysis using the Fine-Gray proportional hazards model. We evaluated the effect of each therapeutics on response using a logistic regression model.
[Results]
We enrolled 2,430 patients [median age at HSCT, 50 (range: 16-74) years] from 14 institutes. Overall, 1,234 patients were transplanted for acute myeloid leukemia or myelodysplastic syndrome, followed by acute lymphoblastic leukemia (n = 381) and non-Hodgkin lymphoma (n = 351). Overall, 1,219 patients (50.2%) had advanced disease (non-remission status) at HSCT. The HCT-CI score was higher (≥3) in 213 patients (8.8%), and 360 (14.8%) were transplanted at poorer performance statuses (PS 2-4). In total, 471 patients (19.4%) received related bone marrow transplantation (BMT), 423 (17.4%) received related peripheral blood stem cell transplantation (PBSCT), 871 (35.8%) unrelated-BMT, and 665 (27.4%) unrelated cord blood transplantation. HLA was mismatched in 1,461 (60.1%) patients.
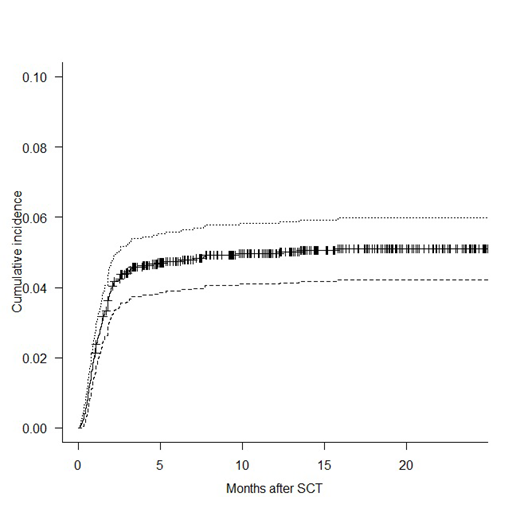
After HSCT, TA-TMA was observed in 123 patients; the cumulative incidence of TA-TMA 12 months after HSCT was 5.0%; TA-TMA occurred at a median of 36 days (range: 3-482) (Figure 1). TA-TMA was correlated with a remarkably inferior OS [hazard ratio (HR), 4.93; 95% confidence interval (CI), 4.03-6.02; P < 0.001] when treating TA-TMA as a time-dependent covariate. In the multivariate analysis, poorer PS [HR, 1.64; 95% CI, 1.05-2.58; P = 0.03], higher HCT-CI [HR, 1.70, 95% CI, 1.02-2.83; P = 0.04], and HLA-mismatch [HR, 2.06; 95% CI, 1.34-3.17; P = 0.001] were significant pre-transplantation risk factors for TA-TMA. Post-transplantation factors (acute GVHD (Grade 3-4) [HR, 2.51; 95% CI, 1.64-3.85; P < 0.001] and veno-occlusive disease (VOD/SOS) [HR, 3.70; 95% CI, 2.05-6.70; P < 0.001]) were also significant risk factors for TA-TMA in the multivariate analysis. No infections (bacterial, viral, or fungal) were significantly related to TA-TMA incidence.
Regarding therapeutic interventions, 36 (29.3%) patients received rTM-including treatment, 6 (5%) were treated with rTM alone, and 30 (24.4%) were treated with rTM and FFP (14; 11%), PE (5; 4%), or both FFP and PE (11; 9%). No significant differences in response rate [OR, 0.99; 95% CI, 0.39-2.52; P = 0.98] and OS [HR, 0.93; 95% CI, 0.58-1.49; P = 0.77] between the groups treated with or without rTM were identified. The results showed similar trends in other therapeutic interventions.
[Conclusion]
This study clarified the incidence of TA-TMA, its impact on clinical outcomes, risk factors including post-transplantation factors, and therapy efficacies. Patients with poor PS, high HCT-CI scores, and HLA-mismatched donors were high-risk patients; the development of severe acute GVHD and VOD/SOS also increased the risk of TA-TMA. rTM administration or other treatments did not improve patient outcomes. Therefore, strategies to avoid TA-TMA are essential. Intensification of the GVHD and VOD/SOS prophylaxis or treatment for these high-risk patients may reduce TA-TMA and improve HSCT outcomes.
Imada:Novartis Pharma K.K.: Honoraria; Takeda Pharmaceutical Co.,LTD.: Honoraria; Celgene K.K.: Honoraria; Bristol-Meyer Squibb K.K.: Honoraria; Otsuka Pharmaceutical Co., Ltd.: Honoraria; Ono Pharmaceutical Co., Ltd.: Honoraria; Kyowa Hakko Kirin Co., Ltd.: Honoraria; Astellas Pharma Inc.: Honoraria; Nippon Shinyaku Co.,Ltd.: Honoraria; Chugai Pharmaceutical Co., Ltd.: Honoraria. Takaori-Kondo:Kyowa Kirin: Research Funding; Chugai: Research Funding; Takeda: Research Funding; Ono: Research Funding; Novartis: Honoraria; Celgene: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria, Research Funding; Janssen: Honoraria; Pfizer: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal