

Introduction
Allogeneic Hematopoietic Cell Transplantation (allo HCT) is currently the only curative therapy for high-risk hematologic malignancies due to the immune response of the donor cells against the malignant cells (graft versus tumor effect; GVT), but with the cost of Graft Versus Host Disease (GVHD). Despite extensive research, very few predictors of GVHD and GVT have been identified to date. Additionally, clinical GVHD diagnosis can be challenging due to chemotherapy-related or infection-related organ toxicity manifestations, which further complicate prediction and treatment stratification algorithms.
In order to study the mechanisms of GVHD and GVT and to identify potential GVHD markers we apply a novel approach, called Transcriptome Fingerprint Assay (TFA), relying on high frequency sampling and blood transcript profiling. The TFA is a multiplex microfluidics q-PCR based assay linked with a computational model for modular functional transcriptome analyses, uniquely tailored to answer complex questions on immune perturbations through frequent profiling of gene expression signatures from < 1 ml of blood (Chaussabel and Baldwin. Nat Rev Immunol 2014, Speake et al. Clin Exp Immunol 2017). This approach has been successfully applied to stratify patients' prognosis in autoimmune and infectious diseases (Banchereau R et al. Cell 2016, Dunning et al. Nat Immunol 2018). In our study we use the TFA to capture longitudinal immune signatures as dynamic "snapshots" of the patient's immune system after HCT.
Hypotheses
Fluctuations over-time in gene expression of allo HCT patients' immune system reflect the pathologic/disease control programs (GVHD/GVT) and may be used to identify diagnostic and predictive biomarkers.
GVHD/GVT control immune programs depend on the "inner" interface between the donor immune-system and the recipient, and are influenced by external variables, as infections or drugs. These variables can affect the immune system-related gene expression and can be measured.
Objectives
To systematically measure gene expression signatures in immune perturbations post-allo HCT, in order to:
Identify GVHD-related immune signatures consistent with clinical diagnosis of GVHD.
Predict and stratify therapy-resistant GVHD and severe chronic GVHD, according to immune signatures.
Identify links (causative and consequential) between GVHD, GVT, relapse, and other post-transplant immune perturbations (e.g. infections).
Methods
Enroll 250 allo HCT patients to populate a "GVHD cohort" and a "non-GVHD cohort" of 50 patients each, and 50 donors (healthy controls cohort) . Patients donate micro-quantities of blood (50 to 600 microliters), weekly until day 100 post-transplant and every 2 weeks thereafter until 2 years after transplant. Detailed clinical, laboratory and therapy annotations are captured during the follow-up. Gene expression of 264 immune-related genes for each sample are measured through Fluidigm BioMark high throughput qPCR system, and normalized to the geometric mean Ct of 8 housekeeping genes. Data interpretation is performed through TFA modular analyses and correlated with the clinical annotations.
Results
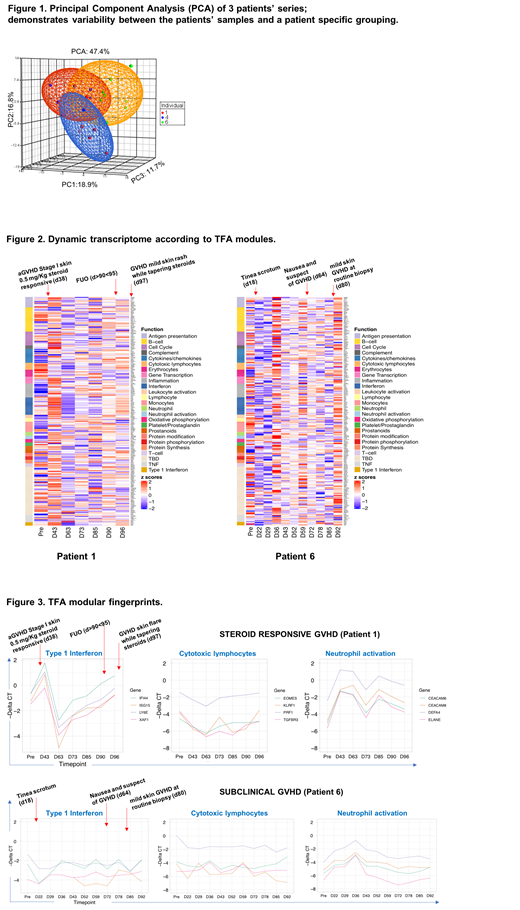
Results of three series of patients' samples are shown to exemplify the potential of TFA as a method to study the mechanisms of GVHD and GVT. All three patients underwent myeloablative peripheral blood stem cell transplant from an HLA identical sibling donor. Two patients developed steroid responsive-acute GVHD (patient #1: GVHD stage I was diagnosed on day 38 post HCT, patient #4: GVHD stage III was diagnosed on day 21 post HCT). One patient (Patient #6) did not develop clinical GVHD, but routine skin biopsy on day 80 revealed apoptotic cells consistent with subclinical skin GVHD. Principal Component Analysis (PCA) of the three patients' series is shown in Figure 1, the dynamic transcriptomes according to TFA modules of patients #1 and #6 are shown in Figure 2, and representative TFA modular fingerprints are shown in Figure 3.
Conclusion
We anticipate that using the TFA approach will help to fill knowledge gaps instrumental to solve clinical dilemmas related to allo HCT complications, and to improve the clinical outcomes of allo HCT patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal