

Introduction: Allo-HSCT was performed on 1771 US children in 2016. SR aGVHD is a life-threatening complication of allo-HSCT associated with substantial healthcare costs and significant reductions in pediatric QOL. Grade II-IV aGVHD occurs in 39-59% of allo-HSCT recipients. While steroids are typically used 1st line, there is no formal 2nd line consensus. RUX has been approved in SR aGVHD patients ≥12 yrs based on results of a single-arm P2 REACH 1 trial where the lower limit of the age range was 18 yrs per the FDA label. The 12 yr age limit of FDA approval was based on a bioequivalence study. Indirect comparisons of RUX trial data vs novel late stage investigational therapies with exclusively pediatric trial data can thus inform future coverage decisions and budget assessments. Recently, a single-arm P3 trial reported efficacy and safety outcomes with REM (investigational agent) in pediatric SR aGVHD. As there are no head-to-head studies comparing RUX to REM, we compared efficacy and safety outcomes between treatments in a statistically robust manner to aid clinical and reimbursement decisions.
Methods: Following NICE Decision Support Unit STC guidelines, regression techniques were used to adjust individual patient-level data from the REM P3 trial to mutually reported baseline (BL) characteristics from the RUX FDA Package Insert (PI)/REACH 1 trial data (2018 ASH Abstract #601). The stepwise model included adjustment for: ethnicity (white), aGVHD grade, and sex. Outcomes of interest included 28-day ORR, 28-day ORR in patients with grade III-IV aGVHD at baseline (BL) from comparable populations (n=49 RUX FDA PI/ n=55 REM), and TEAEs of any grade mutually reported in RUX published data (REACH 1 )/REM trial data (n=71 RUX REACH 1 /n=54 REM). Since the REM trial was limited to pediatric patients, and the youngest patient was 18 yrs in the RUX trial, statistical adjustment for age was unfeasible. Based on RUX approval in patients ≥12 yrs, we assumed that trial populations were comparable despite age differences. Within the REM study, no statistical association was found between age and 28-day ORR or safety in univariate analysis, further validating this assumption. The lack of statistical adjustment for age is, however, a limitation of this analysis. Further limitations include the small sample size of both trials and the small number of endpoints available in the RUX label for comparison.
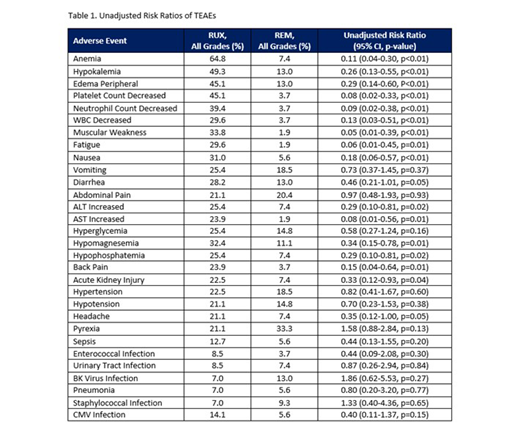
Results: In the full population set for 28-day ORR, the RR of REM vs. RUX was calculated as 1.21 (95% confidence interval [CI], 0.90-1.63; p=0.21) without any covariate adjustment based on ORRs of 69.1% and 57.1% (n=49 RUX FDA PI), respectively. After multivariate adjustment for baseline characteristics, the RR was 1.13 (95% CI, 0.83-1.54; p=0.45). For the BL grade III-IV aGVHD patient subgroup, the unadjusted RR for 28-day ORR of REM vs RUX was 1.72 (95% CI, 1.12-2.63; p=0.01) based on ORRs of 71.4% and 41.6%, respectively. After multivariate adjustment for baseline characteristics, the RR was 1.58 (95% CI, 1.02-2.44; p=0.04), a statistically significant difference. The most frequently reported TEAEs (all grades) for REM were pyrexia (33.3%), abdominal pain (20.4%) and adenovirus infection (20.4%) and for RUX (n=71 RUX REACH 1) were anemia (64.8%), hypokalemia (49.3%) and platelet count decreased (45.1%). AEs led to treatment discontinuation for 15% of patients on REM and 31% on RUX. For mutually reported TEAEs, unadjusted comparisons were employed, as the number of events was too low to facilitate meaningful covariate adjustment. The rates of TEAEs, as well as RRs (95% CI, p-value), are presented in Table 1.
Conclusion: Without direct trial comparison, STC results can be used in cost-effectiveness analyses to aid coverage decisions. STC methods showed significant association of REM with improved 28-day ORR for patients with BL grade III-IV aGVHD (p=0.04) and improved safety outcomes relative to RUX (p<0.05 for RR) for multiple TEAEs, including several hematologic TEAEs (anemia, WBCs, platelets, neutrophils), several lab results (hypokalemia, hypomagnesemia, increased AST), peripheral edema, muscular weakness, nausea, back pain, and fatigue. For all grade 28-day ORR, REM-treated patients experienced relative-but not statistically significant-improvement.
Westley:Mesoblast: Consultancy. Tomaras:Mesoblast: Consultancy. Strati:Mesoblast: Employment. Skerrett:Mesoblast: Employment. Forsythe:Mesoblast: Consultancy. Tremblay:Mesoblast: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal