

The use of post-transplant cyclophosphamide (PTCy) in the context of haploidentical stem cell transplant (haplo-SCT) has led to drastically reduced rates of Graft-vs-Host (GvH) disease through selective depletion of highly allo-reactive donor T-cells. Early trials utilized a reduced-intensity Flu/Cy/TBI preparative regimen and bone marrow grafts; however, relapse rates remained relatively high (Luznik et al. BBMT. 2008). This led to the increased use of myeloablative (MA) regimens for haplo-SCT, which have been associated with decreased relapse rates (Bashey et al. J Clin Oncol. 2013). Most studies have used a MA total body irradiation (TBI) based regimen for haplo-SCT. Preparative regimens using fludarabine and melphalan (FluMel), with or without thiotepa, ATG, and/or low dose TBI have also been reported using bone marrow grafts. Reports on the safety and toxicity of FluMel in the haplo-SCT setting with PTCy and peripheral blood stem cell (PBSC) grafts are lacking. In this two-center retrospective analysis, the safety/toxicity of FluMel as conditioning for haplo-SCT was evaluated. We report increased early mortality and toxicity using standard FluMel conditioning and PBSC grafts for patients undergoing haplo-SCT with PTCy.
38 patients at the University of Rochester Medical Center and the Washington University School of Medicine underwent haplo-SCT with FluMel conditioning and PBSC grafts between 2015-2019. Outcomes were measured by retrospective chart review through July 2019. 34 patients (89.5%) received FluMel(140 mg/m2). Two patients received FluMel(100 mg/m2) and two patients received FluMel(140 mg/m2) + ATG.
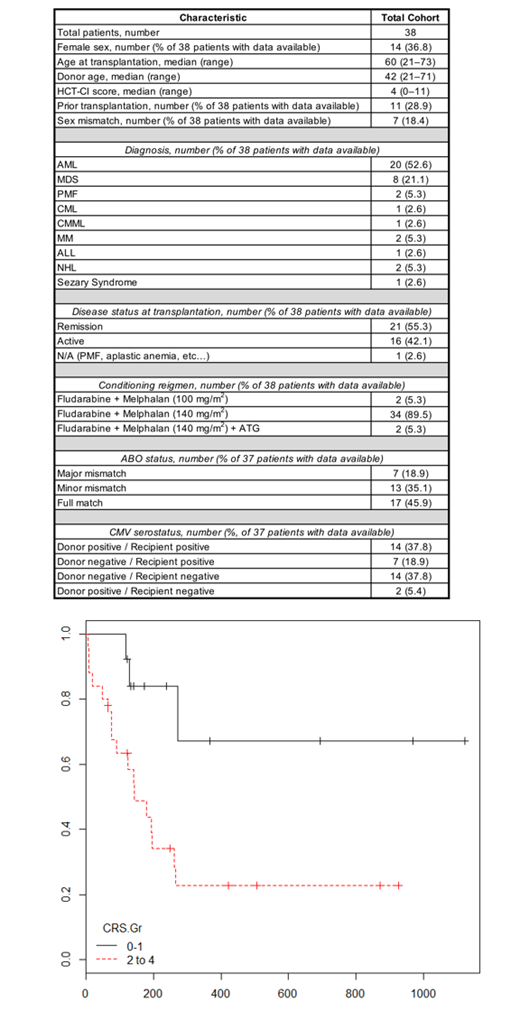
The median age at time of haplo-SCT was 60 years (range 21-73). 20 patients were transplanted for AML, eight for MDS, two for PMF, two for NHL, and five for other malignancies. The median Hematopoietic Cell Transplantation-specific Comorbidity Index (HCT-CI) score was 4 (≥3 indicates high risk). 11 patients had a history of prior stem cell transplant, and 16 patients had active disease prior to their haplo-SCT. Seven patients had sex mismatch with their stem cell donor. Median donor age was 42 (range 21-71).
20 patient deaths occurred by July 2019 with a median follow up of 244 days for surviving patients. Nine patients died before day +100 (D100, "early mortality"), with a D100 non-relapse mortality (NRM) rate of 24%. Median overall and relapse free survival (OS and RFS, respectively) were 197 days (95% CI 142-not reached) and 180 days (95% CI 141-not reached), respectively, for the entire cohort. The 1 year OS and NRM were 29% and 50%. The incidence of grades 2-4cytokine release syndrome (CRS) was 66%, and 52% of these patients were treated with tocilizumab. CRS was strongly associated with early mortality, with D100 NRM of 36% in patients with grade 2-4 CRS compared to 0% in those with grade 0-1. The incidence of acute kidney injury (AKI) was 64% in patients with grade 2-4 CRS, and 8% in those without (p < 0.001). 28% of patients with AKI required dialysis. Grade 2-4 CRS was seen in 54% of patients in remission prior to haplo-SCT and in 92% of those with active disease (p = 0.02).
Of the 9 patients with early mortality, 89% had AKI, 44% needed dialysis, and 100% had grade 2-4 CRS, compared to 31%, 10%, and 55% in those without early mortality (p = 0.002, p = 0.02, p = 0.01). Early mortality was not significantly associated with age, HCT-CI score, second transplant, disease status at transplant, total dose of melphalan, volume overload/diuretic use, or post-transplant infection.
In conclusion, we observed a very high rate of NRM with FluMel conditioning and PBSC grafts for haplo-SCT with PTCy. The pattern of toxicity was strongly associated with grade 2-4 CRS, AKI, and need for dialysis. These complications may be mediated by excessive inflammation in the context of allo-reactive donor T-cell over-activation. Consistent with this, multiple groups have shown that FluMel conditioning in haplo-SCT is safe when using bone marrow or T-cell depleted grafts. Based on our institutional experiences, we would discourage the use of FluMel as conditioning for haplo-SCT with PTCy with T-cell replete PBSC grafts. Alternative regimens or variations on melphalan-based regimens, such as fractionated melphalan dosing or inclusion of TBI may improve outcomes but further study and randomized controlled trials are needed. This study is limited in its retrospective design and sample size.
DiPersio:WUGEN: Equity Ownership, Patents & Royalties, Research Funding; Karyopharm Therapeutics: Consultancy; Magenta Therapeutics: Equity Ownership; Celgene: Consultancy; Cellworks Group, Inc.: Membership on an entity's Board of Directors or advisory committees; NeoImmune Tech: Research Funding; Amphivena Therapeutics: Consultancy, Research Funding; Bioline Rx: Research Funding, Speakers Bureau; Macrogenics: Research Funding, Speakers Bureau; Incyte: Consultancy, Research Funding; RiverVest Venture Partners Arch Oncology: Consultancy, Membership on an entity's Board of Directors or advisory committees. Liesveld:Onconova: Other: Data safety monitoring board; Abbvie: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal