

Background: Our institutional HSCT Program was formally established in 1986, performing 33 transplantations throughout the following decade, obtaining an overall survival (OS) of 28% and a high non-relapse mortality (NRM) (61%) in allogeneic hematopoietic stem cell transplantation (allo-HSCT). According to these unfavorable results, in 1998 our program was restructured with the consequent development of a modified HSCT method (reduced BuCy 2) adapting to our limited resources with the objective of decreasing the NRM and improving the OS.
Objective: To describe the outcomes of allo-HSCT using reduced BuCy 2 as conditioning regimen in a Mexican referral center.
Patients and Methods: A retrospective study was performed including consecutive patients undergoing allo-HSCT at the National Institute of Medical Sciences and Nutrition Salvador Zubiran, from May 1999 to May 2019. Data was obtained from a prospectively created database. Reduced BuCy 2 consisted of busulfan 12 mg/kg, ORAL and cyclophosphamide 80mg/kg, IV. Therapeutic busulfan monitoring was not available. Cyclosporine A (CsA) and methotrexate (MTX) were given for GVHD prophylaxis. Blood products, nutritional support, and antimicrobial prophylaxis were provided according to institutional guidelines. Disease risk index (DRI) was classified as low, intermediate or high using standard definitions and the HCT-CI score was assigned to each patient. Morbidity post-transplant was analyzed through the toxicity evaluation according to the NCI CTCAE v4.0, which classifies each toxicity as grades I-IV. Veno-occlusive disease (VOD) was diagnosed according to the modified Seattle criteria. Graft-versus-host disease (GVHD) was evaluated according to NIH guidelines. Endpoints included OS and NRM. Descriptive statistics were used. Kaplan-Meier curves were used to analyze survival using SPSS v.21.
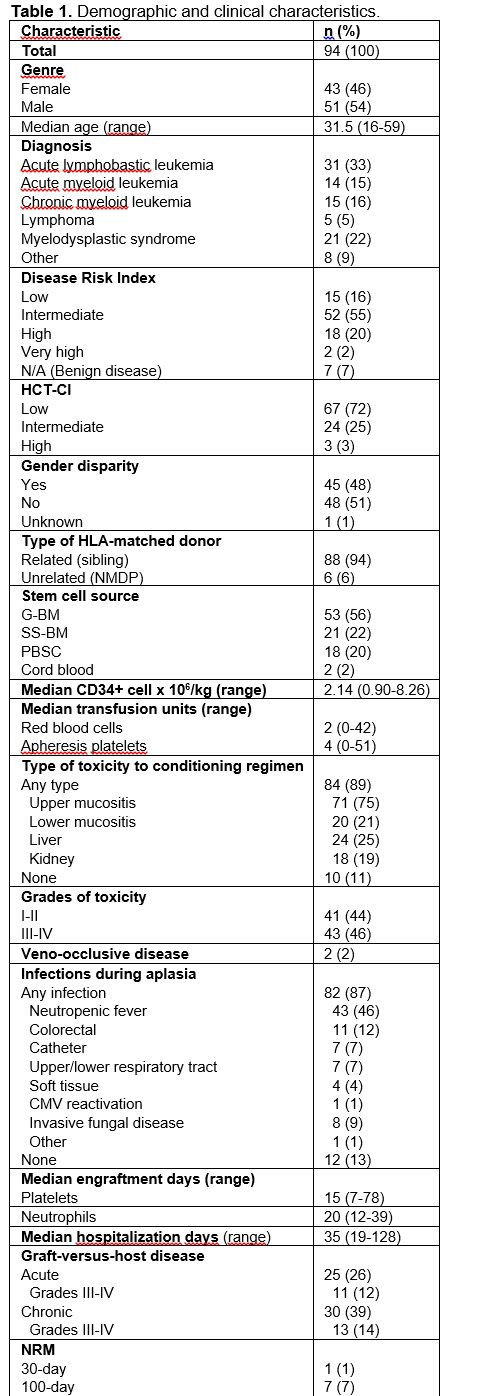
Results: Ninety-four patients were included. Table 1 shows patient and HSCT characteristics. Most were males (54%) and the median age was 31.5 years. The most common diagnosis was acute lymphoblastic leukemia (ALL) (33%), followed by myelodysplastic syndrome (MDS) (22%), and Chronic myeloid leukemia (CML) (16%). Most patients had an intermediate DRI (55%) and the HCT-CI score was mostly low (72%). Only 6% of allo-HSCT used a matched unrelated donor. The most frequent source of HSCs was G-CSF-primed bone marrow (56%). Toxicity to the chemotherapy regimen was observed in 89%, from which 48% were grades III-IV. VOD was observed in 2 patients. Most common infections included neutropenic fever (46%) and colorectal affection (12%). Invasive fungal disease was observed in 9% and CMV reactivation in 1%. Median days of engraftment were 15 and 20 for platelets and neutrophils, respectively. No engraftment failure was observed. Acute and chronic GVHD was observed in 26% (88% grades I-II) and 39% (86% limited disease), respectively. Thirty and 100-day NRM was 1% and 7%, respectively. Ten-year OS was 54% for all the cohort and the most frequent cause of death was relapse (61%) followed by GVHD (26%), and infections (13%); by disease, it was as follows: ALL 30%, acute myeloid leukemia 57%, CML 64%, lymphomas 33%, MDS 85%, and others 50%.
Conclusion: Reduction in NRM has been of interest in allo-HSCT over the years, requiring more effective strategies. Since 1998, we have used an adjusted conditioning method for allo-HSCT due to the high toxicity and mortality related to conventional BuCy2 at the beginning of our HSCT Program. Our regimen consists of reducing conventional BuCy2 (˂ 25% of Bu and ˂ 20% Cy), preserving its myeloablative potential, considering reduced tissue injury, and therefore, reduced systemic toxicity; consequently maintaining immunosuppression for fast engraftment, and reducing NRM. Mucositis was the main toxicity but it resolved with supportive care. Grade III-IV aGVHD was low (12%), as well as extensive cGVHD (14%). Thirty and 100-day NRM was very low. The findings of our study demonstrate that reduced BuCy2 regimen associates with minimal morbi-mortality and might represent an alternative for conditioning in the allo-HSCT context, especially in limited resource centers at developing countries were novel agents and total body irradiation are not available.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal