

Background: Patients with lymphoma and myeloma undergoing autologous hematopoietic stem cell transplantation (ASCT) are at risk for mobilization failure, defined as the inability to harvest the minimum recommended 2x106/kg CD34+ cells prior to conditioning. This limitation can be surpassed by combining multiple apheresis sessions, cryopreservation and adding plerixafor to filgrastim. However, these strategies substantially increase transplant costs and are unaffordable for many patients in low and middle-income countries (LMIC). Furthermore, standard doses of plerixafor can lead to unnecessarily high CD34+ cell yields, leading to resource waste. We have previously shown that a reduced dose of plerixafor at 0.12 μg/kg is effective in a pilot trial. Consequently, we have incorporated RD-plerixafor to a mobilization algorithm using peripheral CD34+ cell analysis to be used in a setting with limited resources.
Objective: To evaluate the efficacy of a decision-making mobilization algorithm in patients with lymphoma or myeloma defined by our ability to harvest at least 2x106Kg CD34+ cells in a single apheresis session.
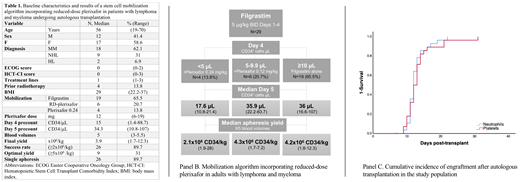
Methods: We performed a single-arm prospective study including consecutive adults diagnosed with lymphoma or myeloma undergoing ASCT in our institution. Patients received a mobilization regimen consisting of filgrastim 5 μg/kg BID for 4 days. On day 4 peripheral blood CD34+ cell flow cytometry analysis was performed. We designed a mobilization algorithm hypothesizing that if the day 4 CD34+ pre-count was 5-10 cells/μL, a single RD-plerixafor dose at 0.12 mg/kg (11 hours prior to apheresis) would be sufficient to achieve a successful harvest (≥2x106/kg CD34+) in one large-volume apheresis session based on a prior local study (Panel B). Patients with <5 cells/μL received filgrastim plus a single dose of plerixafor 0.24 mg/kg and those with ≥10 cells/μL received filgrastim alone. Plerixafor vials were shared between 2 patients when possible. Day 5 peripheral CD34+ cell analysis was also performed. Cells were not frozen but were stored at 4ºC. Adverse effects, final CD34+ yield and probability of engraftment using 1-survival Kaplan Meier analysis were determined. This study was performed in accordance to the Declaration of Helsinki.
Results: Twenty-nine patients were included. Baseline characteristics and outcomes are shown in Table 1. Median day 4 CD34+ cell pre-count was 15 cells/μL (range, 1.4-88.7). Following our algorithm n=19 patients received filgrastim (65.5%), n=6 received RD-plerixafor (20.7%) and n=4 full-dose plerixafor (13.8%). Median day 5 peripheral blood CD34+ increased to 34.3 cells/μL (range, 10.8-107) (Wilcoxon signed ranked p<0.001), with a median increase of +28 cells/μL (+16.77-55.8) in the RD-plerixafor group. No severe adverse events were observed. We were able to successfully harvest 89.7% of patients using our algorithm with median final yield of 3.9x106 (1.7-12.3) CD34+cells/kg. Mobilization success rates were 94.7% for patients who recieved filgrastim alone, 83.3% for RD-plerixafor and 75% for full-dose plerixafor-treated patients. Optimal yields (≥5x106/kg) were achieved by 31% of patients using our strategy. Only three required a second apheresis session, and all underwent successful outpatient transplantation. One patient died due to hemorrhagic stroke on day +7. All remaining patients engrafted. Median probability of engraftment was estimated at 12 days for both neutrophils (95% CI 11.4-12.6) and platelets (95% CI 11.1-12.9) (Panel C). Female sex and prior treatment lines (continuous) were significantly associated to plerixafor requirement in a univariate regression analysis. Our strategy led to savings of $22,000 USD by lowering the plerixafor dose alone.
Conclusion: Incorporating RD-plerixafor into a mobilization algorithm is a safe and effective strategy that increases access to transplantation in patients with lymphoma and myeloma at risk of harvesting failure. External validation of our decision-making algorithm is warranted.
Gomez-Almaguer:Amgen: Consultancy, Speakers Bureau; Janssen: Consultancy, Speakers Bureau; Teva: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Celgene: Consultancy, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal