

Background: G-CSF-primed bone marrow (G-BM) is used in some centers as the product of choice in related donor transplants because of lower rates of GVHD and fast engraftment (Morton 2001; Deotare et al. 2015). Marrow collections substantially diluted with peripheral blood may, however, compromise the GVHD-sparing effect of G-BM. Concerns over the variability in the quality of bone marrow harvest have been reported (Spitzer et al. 1994; Prokopishyn et al. 2019). We explored the role of a simple novel quality indicator, i.e peripheral blood to marrow harvest WBC ratio, as a predictor of GVHD risk.
Materials and methods: We analysed 156 successive bone marrow harvests for patients suffering from severe thalassemia using G-BM donated by fully matched (10/10 or 12/12) related donors (143 siblings and 13 mothers) at Sankalp-People Tree Centre for Paediatric BMT - Bangalore (80 patients) and Sankalp-CIMS Centre for Paediatric BMT - Ahmedabad (76 patients).
G-CSF priming was done for 5 days before the transplant with 10 mcg/kg/day in 2 divided subcutaneous doses and peripheral counts were obtained within 24 hours of collection. G-BM was collected in bags with 20 ml 50 U/ml heparin for the first 200 ml and further 10ml/100ml of marrow. We defined quality of marrow as follows:
Quality of Marrow = WBC count of G-CSF primed BM / Peripheral WBC count of donor
Quality of Marrow < 0.9 was categorised as poor as it signifies that the concentration of WBCs in bone marrow is same or lesser than the pre-harvest peripheral counts. EBMT criteria was used for grading GVHD. We calculated the odds of aGVHD based upon the quality of marrow. Beside marrow quality, the sex of the recipient seemed to impact GVHD rates and thus regression analysis was used to study the impact of G-BM quality independent of other factors.
Statistics were performed on R software (version 3.5.x). Mann Whitney and Fisher's exact tests were used to compare numeric and categorical data respectively.
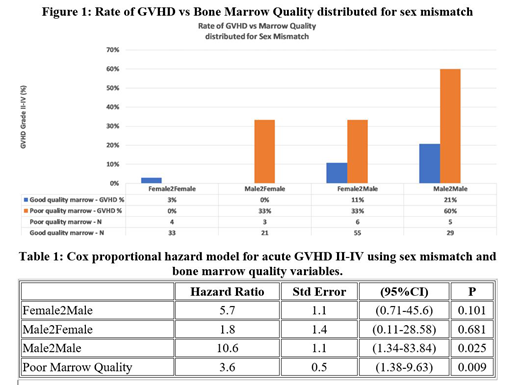
Results: Of the 156 harvests, 18 had poor marrow quality; 33% (6 of 18) of these developed acute GVHD grade II-IV as opposed to 9% (13 of 138) (see Figure 1). Between those who developed GVHD and those who did not, marrow quality (p=0.012), patient sex (p=0.006) and sex mismatch status (p=0.014) were significantly different. Differences in total cell dose (p=0.65), transplant centre (p=0.62), bone marrow cell count (p=0.14) and peripheral cell count before harvest (p=0.72), donor age at BMT (p=0.42), relationship with the donor (p=1.0) and average volume of marrow per draw of syringe (p=0.23) showed no statistical significance.
Variables with significant difference (sex mismatch and bone marrow quality) were entered in the Cox's proportional hazards model for acute GVHD II-IV which showed that poor marrow quality is the most significant independent risk associated with a hazard ratio of 3.6 (p=0.009), followed by male to male transplants which were associated with a hazard ratio of 10.6 (p=0.03) See Table 1.
Further, poor quality marrow was associated with lower cell count in marrow (p<0.001), higher peripheral counts (p<0.001), higher collection volume (p=0.035) and was seen more in one centre compared to the other (p<0.001). Donor age (p=0.81), donor's relationship (p=1.0), donor sex (0.62), donor's carrier status (p=0.64), donor weight (p=0.85) and average volume of marrow per draw of syringe (p= 0.76) were not statistically significant.
Discussion: The role of tolerance induced by mesenchymal stem cells in reduction (Aggarwal 2005) and even the treatment of GVHD (Le Blanc et al. 2004; Baron and Storb 2012) has been reported elsewhere and supports our findings though this is yet to be established (Fisher et al. 2019). Simple quality control of BM could be highly beneficial in all settings in minimising acute GVHD. This is particularly important in low- and middle-income countries where GVHD can be very challenging (Saleem et al. 2018) and is associated with high costs of management and prolonged hospitalisation (Grubb et al. 2016). Our indicator is accurately measurable, inexpensive, precise and timely; further it does not involve any sophisticated equipment (flow cytometry for CD counts), thus may be widely applicable and usable.
Conclusion: Quality of BM harvest, as indicated by PB to BM WBC ratio, is a simple, effective and inexpensive informative indicator in the context of G-BM. Poorer quality of marrow collection may be contributing to increased risk of acute GVHD.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal