

Background: Small lymphocytic lymphoma/chronic lymphocytic leukemia (SLL/CLL) is a lymphoproliferative disorder of small mature B-cells, most commonly presenting with peripheral blood and bone marrow involvement. Tumoral lesions are variably encountered, resulting from either lymph node involvement or, less commonly, infiltration into virtually any extramedullary site. The prognostic assessment of patients with SLL/CLL relies strongly on the identification of recurrent chromosomal abnormalities, which are routinely tested by fluorescence in situ hybridization (FISH) on peripheral blood or bone marrow specimens. However, the incidence of such recurrent chromosomal abnormalities on tumoral lesions has only been studied on small series, and its concordance with peripheral blood and/or bone marrow testing remains unknown. We hereby report a large series of chromosomal abnormalities detected on tumoral SLL/CLL lesions, based on a validated FISH panel for formalin-fixed/paraffin-embedded (FFPE) biopsy sections.
Methods: FISH was performed at Mayo Clinic on FFPE tissue sections from biopsies obtained from May 2014 to November 2018, as clinically indicated. Pathology reports and H&E-stained sections were reviewed and were consistent with a diagnosis of SLL/CLL in all cases. Probes were validated to detect previously described chromosomal abnormalities in SLL/CLL, including trisomy 12 (+12) and deletions of 6q23 (6q-), 11q22.3 (11q-), 13q14.3 (13q-) and 17p13.1 (17p-). Available FISH results performed on peripheral blood or bone marrow samples from these patients were also reviewed for comparison.
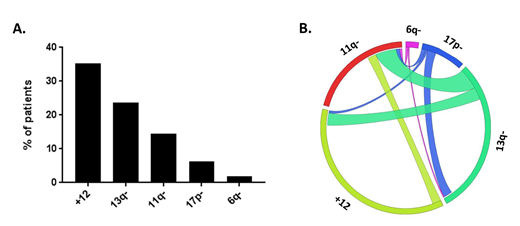
Results: Tissue biopsies involved by SLL/CLL from 346 patients were evaluated by FISH. The majority of specimens were either lymph nodes (65%) or soft tissue masses (29%). The median age was 66.9 years (range: 36 to 91), and the male to female ratio was 2.1:1. FISH abnormalities were identified in 60% of evaluated tissue sections. The most frequently detected aberration was +12 (35%), followed by 13q- (24%), 11q- (15%), 17p- (6%) and 6q- (2%) (Figure A). In particular, the incidence of +12 was significantly higher, and the incidence of 13q- significantly lower compared to frequencies previously reported on peripheral blood or bone marrow specimens (p<0.01 for both abnormalities, in comparison to a recently published cohort of 1585 patients: Br J Haematol 2016;173:105). Most cases had 1 abnormality (55%), with fewer patients having 2 abnormalities (13%), and only 1 case showing 3 abnormalities. Of 47 patients with 2 or more chromosomal aberrations, most (72%) had 13q- in combination with either 11q- (7 cases), +12 (10 cases) or 17p- (7 cases) (Figure 1B). Of 29 patients with positive blood or bone marrow FISH results within 12 months of tissue biopsy, 7 patients (24%) had discrepant results, all of which were limited to discordant +12 and/or 13q- detection. In 14 additional patients with positive blood or bone marrow FISH results more than 12 months before or after tissue biopsy, discordant results were found in 3 cases (21%), all of which indicated gains of 17p- (2 cases) or 11q- (1 case) on the follow-up analysis.
Conclusions: We hereby report the largest documented series (to the best of our knowledge) of FISH results performed on tumoral lesions of SLL/CLL. Trisomy 12 was overrepresented in tumoral lesions, as compared to the reported predominance of 13q- in leukemic involvement. Discrepant results between concurrent tumoral and leukemic FISH testing were limited to differences in +12 and 13q- in our series. We also document the acquisition of aberrancies of unfavorable prognosis (17p- and 11q-) on follow up FISH analysis in a small subset of patients, which should be taken into account when considering repeat FISH studies.
Horna:MorphoSys AG: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal