

The majority of patients with myelodysplastic syndromes (MDS) require regular red blood cell (RBC) transfusions. Alloimmunization (AI) against blood products is an adverse event, causing time-consuming RBC compatibility testing. The reported incidence of AI in MDS patients varies greatly. Even though different studies on AI in MDS patients have been performed, there are still knowledge gaps. Current literature has not yet fully identified the risk factors and dynamics of AI in individual patients, nor has the influence of disease modifying treatment (DMT) been explored. Therefore, we performed this study to evaluate the effect of DMT on AI.
An observational, population-based study, using the HemoBase registry, was performed including all newly diagnosed MDS patients between 2005 and 2017 in Friesland, a province of the Netherlands. All available information about treatment and transfusions, including transfusion dates, types, and treatment regimens, was collected from the electronic health records and laboratory systems. Follow-up occurred through March 2019. For our patient cohort, blood products were matched for AB0 and RhD, and transfused per the 'type and screen' policy (i.e. electronic matching of blood group phenotype between patient and donor). After a positive antibody screening, antibody identification and Rh/K phenotyping was performed and subsequent blood products were (cross)matched accordingly. The observation period was counted from first transfusion until last transfusion or first AI event. Univariate analyses and cumulative frequency distributions were performed to study possible risk factors and dynamics of AI. DMT was defined as hypomethylating agents, lenalidomide, chemotherapy and monoclonal antibodies. The effect of DMT as a temporary risk period on the risk of AI was estimated with incidence rates, relative risks (RR) and hazard ratios (HR) using a cox regression analysis. Follow-up was limited to 24 months for the cox regression analysis to avoid possible bias by survival differences. Statistical analyses were performed using IBM SPSS 24 and SAS 9.4.
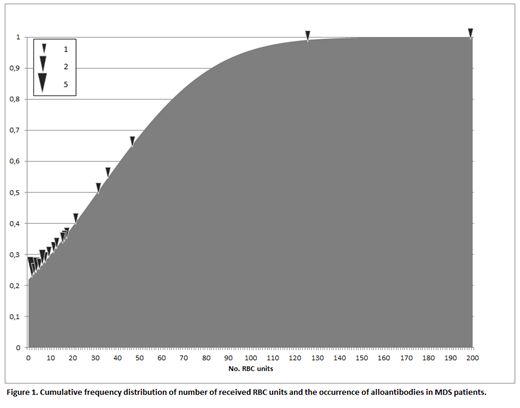
Out of 292 MDS patients, 236 patients received transfusions and were included in this study, covering 463 years of follow-up. AI occurred in 24 patients (10%). AI occurred mostly in the beginning of the observation period: Eighteen patients (75%) were alloimmunized after receiving 20 units of RBCs, whereas 22 patients (92%) showed AI after 45 units of RBCs (Figure 1). We found no significant risk factors for AI in MDS patients at baseline.
DMT was given to 67 patients (28%) during the observation period. Patients on DMT received more RBC transfusions than patients that did not receive DMT (median of 33 (range: 3-154) and 11 (range: 0-322) RBC units respectively, p<0,001). Four AI events (6%) occurred in patients on DMT and 20 AI events (12%) occurred in patients not on DMT. Cox regression analysis of the first 24 months of follow-up showed an HR of 0.30 (95% CI: 0.07-1.31; p=0.11). The incidence rates per 100 person-years were 3.19 and 5.92 respectively. The corresponding RR was 0.54 (95% CI: 0.16-1.48; p=0.26).
Based on our results, we conclude that the incidence of AI in an unselected, real world MDS population receiving RBC transfusions is 10% and predominantly occurred in the beginning of follow-up. Risk factors for AI at baseline could not be identified. Our data showed that patients on DMT received significantly more RBC transfusions but were less susceptible to AI. Therefore, extensive matching of blood products may not be necessary for patients on DMT. Larger studies are needed to confirm the protective effect of DMT on AI.
Rozema:Celgene: Other: Financial support for visiting MDS Foundation conference.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal