

Background: Rituximab combined with chemotherapy (R-chemotherapy) is the standard of care first-line treatment for diffuse large B-cell lymphoma (DLBCL). Despite success with R-chemotherapy, 30% to 50% of patients with high-risk DLBCL will relapse, and outcomes are poor among patients who relapse within one year of diagnosis. Given the challenge of successful salvage, novel first-line therapies are needed. Blinatumomab, a bispecific T-cell engager (BiTE®) antibody construct that directs cytotoxic T cells to lyse CD19-expressing B cells, has shown efficacy as salvage therapy in patients with relapsed or refractory DLBCL. This open-label, multicenter, phase 2 study (ClinicalTrials.gov, NCT03023878) assessed the efficacy and safety of blinatumomab after first-line R-chemotherapy for patients with newly diagnosed, high-risk DLBCL.
Methods: Patients (≥18 y) had proven high-risk DLBCL (International Prognostic Index [IPI] 3−5 and double/triple hit or double MYC/BCL2 expressor) and Eastern Cooperative Oncology group performance status ≤2. To be eligible for blinatumomab, patients were required to achieve complete metabolic response (CMR), partial metabolic response (PMR), or stable metabolic response by PET/CT after a run-in period with 6 cycles of R-chemotherapy (R-CHOP, R-DA-EPOCH, or R-CHOEP). Blinatumomab was given by continuous intravenous infusion in a single 84-day cycle 1 (9 μg/day for 7 days, 28 μg/day for 7 days, and 112 μg/day for 42 days, followed by a 28-day treatment-free interval) and an optional 28-day cycle 2 (9 μg/day for 7 days, 28 μg/day for 7 days, and 112 μg/day for 14 days) for patients without progressive metabolic disease (PMD). The primary endpoint was the incidence and severity of adverse events (AEs). Additional endpoints were objective response rate (ORR [CMR + PMR]) per Lugano criteria, minimal residual disease (MRD) by plasma cell−free circulating tumor DNA, overall survival (OS), and pharmacokinetics (PK).
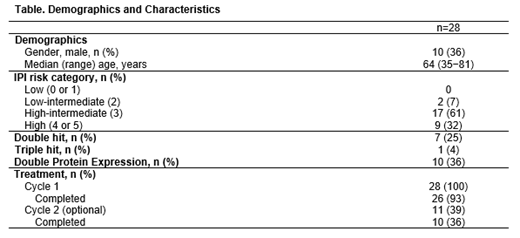
Results: Of 47 patients enrolled, 17 (36%) discontinued R-chemotherapy run-in (protocol criteria, n=6; patient request, n=5; disease progression, n=3; ineligibility, n=1; AE, n=1; death, n=1) and 30 (64%) completed the run-in (2 did not proceed to blinatumomab). Of 28 patients who received blinatumomab, 26 (93%) had high or high-intermediate IPI; 8 (29%) were double/triple hit and 10 (36%) were double protein expressors (Table). In total, 26 (93%) patients completed cycle 1; ten of 11 (91%) patients completed optional cycle 2. Blinatumomab PK were consistent with those in previous studies.
After the R-chemotherapy run-in before starting blinatumomab, 24 patients had objective metabolic responses and 4 had no metabolic response (NMR). After blinatumomab treatment, the ORR (within 12 weeks of starting blinatumomab) was 89% (25/28 patients; 95% CI, 72−98; Table). The 4 patients with NMR before blinatumomab had objective responses after blinatumomab treatment. Three patients with objective responses before blinatumomab relapsed after blinatumomab. Twenty-six (93%) patients were still alive with a median follow-up time of 8.6 months; 2 died (disease progression; n=1; infection not related to treatment, n=1). Nine of 13 (69%) patients during the R-chemotherapy run-in were MRD positive, all of whom converted to MRD negative after treatment with blinatumomab. After treatment with blinatumomab, 17 of 18 (94%) patients were MRD negative; the MRD positive patient had PMD.
During blinatumomab treatment, 11 (39%) patients had grade ≥3 AEs, and 5 (18%) had grade ≥4 AEs. Two (7%) patients discontinued treatment due to AEs (grade 3 neurotoxicity; grade 4 neutropenia). Consistent with previous blinatumomab reports, neurologic events (NEs) were reported in 17 (61%) patients, including 3 (11%) with grade 3 NEs and 1 (4%) with NEs leading to treatment discontinuation. No patients had grade ≥3 cytokine release syndrome. Other grade ≥3 events of interest included neutropenia and febrile neutropenia (n=4; 14%) and infection (n=3; 11%).
Conclusions: In patients with newly diagnosed, high-risk DLBCL, blinatumomab monotherapy after first-line R-chemotherapy led to an 89% ORR, and safety was consistent with that in earlier studies in DLBCL. Thus, blinatumomab is a potential treatment option for patients with newly diagnosed disease.
Katz:Stemline: Speakers Bureau; Dova: Consultancy. Chu:Celgene: Honoraria; Teva: Consultancy; AstraZeneca: Honoraria; Amgen Inc.: Honoraria; Gilead: Honoraria. Thieblemont:Roche: Honoraria, Research Funding; Gilead: Honoraria; Novartis: Honoraria; Kyte: Honoraria; Janssen: Honoraria; Celgene: Honoraria; Cellectis: Membership on an entity's Board of Directors or advisory committees. Morley:Amgen: Membership on an entity's Board of Directors or advisory committees, Other: speaker fees, conference support ; TAKEDA: Other: conference support ; Janssen Pharmaceuticals: Other: speaker fees; ROCHE: Membership on an entity's Board of Directors or advisory committees, Other: conference support; ABBVIE: Other: speaker fees. Chen:Amgen Inc.: Employment, Equity Ownership. Kalabus:Amgen Inc.: Employment, Equity Ownership. Morris:Amgen: Employment, Equity Ownership. Anderson:Amgen Inc.: Employment, Equity Ownership. Avilion:Amgen Inc.: Employment, Equity Ownership. González-Barca:Takeda: Honoraria; Kiowa: Consultancy; Celtrion: Consultancy; Janssen: Consultancy, Honoraria; Celgene: Consultancy; Roche: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal