

Introduction
Estimated incidence of cHL in Argentina is 842 cases/year (Globocan 2018). There is no local data regarding response rates (RR) to FL. GATLA (Grupo Argentino de Tratamiento de Leucemia Aguda) reported 3 years progression free survival (PFS) rates of 90% and overall survival (OS) of 98% regardless of stage. HL has a high cure rate; 10% are primary refractory and 30% relapse after achieving complete remission (CR). In stage I-IIa, 5 years OS is estimated around 90% and 60% in stage IV (Ann Hematol 2019).
Objectives
Primary: To learn the RR, PFS and associated variables after FL of cHL in public (PuI) and private institutions (PrI) in Argentina.
Secondary: To learn the OS rates. To study epidemiological characteristics of the patients (Pts) in participating institutions and reveal differences which may affect the response to treatment.
Materials and methods
Retrospective analysis of consecutive Pts with diagnosis of cHL from 1/1/2008 to 2/1/2019 with available follow up data. Descriptive statistics was performed in clinical variables and histopathological findings. Quantitative variables were expressed as median an interquartile range (IQR) and qualitative variables as total number and percentage (%). Survival rates were estimated by the Kaplan-Meier method and compared by the log-rank test. OS was measured from the date of diagnosis to date of death or last follow-up visit.
Results
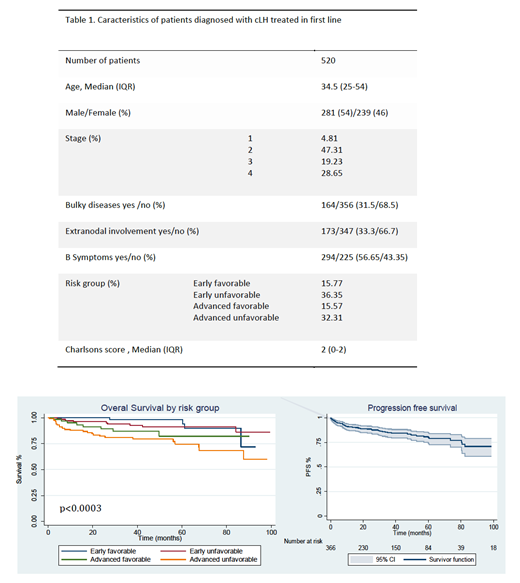
520 Pts from 7 PuI and PrI in Buenos Aires and Rosario were examined. 22 Pts had nodular lymphocyte predominant HL. Data on the 498 Pts with cHL is presented. Median follow up: 37.4 months (CI95% 17.7-63.5). Pts characteristics: Table 1. The median time from diagnosis to FL was 22 days (IQR 14-42), significantly shorter in PrI (32.5 (IC95% 27-38) vs. 49.3 (IC95% 38.5-60.2); p=0.0027). 96.5% of Pts received ABVD as FL, dose modifications or transitory suspension were required in 17.1%, and 82.1% received all cycles properly. CR was achieved in 83.4% of Pts and partial remission (PR) in 6.3%. The % achieving CR was higher in PrI; more PR were achieved in PuI. 10.3% had progressive disease (PD) at the end-of FL. 85.4% (n=373) had negative end-of-treatment FDG-PET results (DS1-3). Interim PET scan was performed in 70% of Pts (n=357), with 83.8% achieving metabolic CR but only 15.5% (n=70) being treated with response-adapted strategies (6.5% deescalated to AVD). Regarding hematologic toxicity, anemia, neutropenia and thrombocytopenia were found in 28.5%, 56.4% and 7.2% of Pts, respectively. Febrile neutropenia was reported in 9 Pts. 28.6% developed non-hematologic toxicities (41/144 pulmonary toxicity). 51 Pts had primary refractory disease and 69 (14%) relapsed during follow-up (median time to relapse 4.4 months (CI95% 0-13)). 65 Pts died (12.5%), 34 due to lymphoma progression and the remaining 31 due to toxicity. 2 years OS rate was 91% (CI95% 88% - 94%) and 85% at 5 years (CI95% 80% - 89%). There was no difference in OS between PrI and PuI (p=0.27); every day of delay in the beginning of FL increased 0.89 (IC95% 0.6-1.8) the risk of achieving PR or PD at the end of FL. 5 years PFS rate was 76% (CI95% 70-81) (figure 1-2: OS according to risk group and PFS). Outcomes were statistically better in women, age younger than 60, non-bulky disease, absence of extranodal disease or risk factors such as leukocytosis, lymphopenia and hipoalbuminemia. Pts with normal ESD, stage I-III, early favorable and advanced favorable stages and Charlson score <3 also showed survival advantage (p<0.01). On multivariate analysis Charlsons score and end-of-treatment FDG-PET scan remained independent predictors of OS with HR of 1.2 (CI95%1.1-1.7; p=0.001) and 2.3 (CI95% 1.7-3.2; p<0.0001), respectively.
Conclusions
This is one of the largest retrospective cohorts reported in cHL. Epidemiology characteristics, RR, PFS, and associated variables are similar to the ones reported in literature. Five years OS proved to be higher than previously reported. ABVD is the chemotherapy regimen of choice in our country and as our study shows, is well tolerated but not exempt from toxicity. Early FL initiation improves outcome. PET scan was widely used but only 15.5% of the Pts were treated with response adapted strategies. Taking into account that in 47.6% of the Pts toxicity was the main cause of death, the use of PET-guided treatment in our population should be strongly considered.
* The first four authors have equal contribution
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal