

Introduction
The best strategy for the follow-up of patients with Hodgkin Lymphoma (HL) in complete remission (CR) after the first line of treatment is not established. The NCCN guidelines recommend follow-up computed tomography scan (CT) at 6, 12 and 24 months after the end of treatment. Several clinical trials of relevance require the follow-up with quarterly CT during the first year after treatment, and every 6 months thereafter. However, these recommendations are based on expert opinion rather than evidence. The aim of our study is to evaluate the different follow-up strategies after 1st line of treatment in patients with diagnosis of LH who achieved CR, and to identify the best follow-up strategy.
Materials and methods
This is a multicenter, retrospective study. We analysed 604 patients from 11 GELTAMO group centers, diagnosed with HL between 2007 and 2016 that had positron emission tomography-computed tomography scan (PET-CT) for initial staging, and at the end of induction treatment. Patients were grouped according to the different follow-up strategies in: 1) only clinical (clinical history, blood test (BT) and physical examination), 2) CT 3) PET-CT. The study was approved by the ethics committee of the Gregorio Marañón hospital. Medians, ranges and percentages were used for the descriptive analysis and the X2 test, Fisher's test and the Mann-Whitney U test for the comparison of variables.
Results:
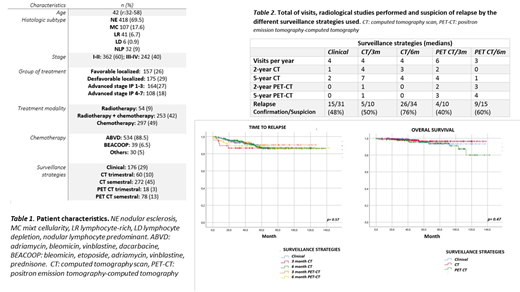
Patients and disease characteristics and treatment information are included in Table 1. Table 2 shows the number of radiological images performed, the number of visits and the suspicion of relapse according to the used strategy. The median follow-up was 64 months (24-180). Of 90 suspicions, 59 relapses were confirmed. Relapse was identified in 64% of the patients by some clinical data that suggested it, 17% of patients had only symptoms, 25% had only abnormal physical examinations, 2% had only abnormal BT and 20% presented a combination of all the clinical variables. Regarding laboratory assessment at relapse time, 62% of the patients had a normal blood test at the time of relapse, 18% had elevated ESR, 8% elevated LDH and 9% abnormal blood count. Regardless of the strategy, 55% of relapses had at least one accessible lesion on physical examination. Comparing the used strategy, the median time to relapse was 19 months (p25-75 = 8-39) for the clinical follow-up, 18 months (p25-75 = 9-41) with CT follow-up and 13 months (p25-75 = 2-23) with PET-CT, with not statistical significance differences among them (p = 0.57) (Figure 1). Overall survival was not different using any of the strategies (Figure 2).
Conclusions:
In our study, the use of CT and PET-CT for the follow-up of patients with HL does not significantly reduce the time to identify the relapse and has no impact on survival. In addition, these strategies expose patients to radiation and have a high cost with not clear benefit. Our next step is to confirm this results with a prospective study.
Vidal Maceñido:GILEAD SCIENCES: Research Funding. Perez De Oteyza:Celgene: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal