

Background: PCGTCL is a rare disorder, accounting for < 1% of all lymphomas. In part given the rarity, timely and accurate diagnosis (dx) remains challenging. Moreover, PCGTCL is typically characterized by a highly aggressive course. We conducted a multi-institutional, retrospective analysis to delineate pathology, patient (pt) characteristics, treatment patterns & outcomes of PCGDTCL in the modern era.
Methods: We collected detailed information on pts with PCGDTCL dx between 2000 - 2017 across 10 academic centers. Pathologic data, including IHC & flow characteristics on de-identified pathology reports, were reviewed centrally by an expert dermatopathologist (MP). A pathologic tier was assigned to each case based on fidelity to the following pre-defined minimum criteria: flow cytometric evidence of gamma and/or delta protein-expressing lymphoma or histopathologic evidence of gamma and/or delta protein expression & at least 50% atypical lymphocytes positive for gamma/delta immunostain (IHC) with tissue representative of entire lesion. The presence of >25% CD30 positivity of malignant lymphocytes was an exclusion criterion. Further, PCR evidence of TCR gamma monoclonality or TCR beta/betaF1 negativity alone were inadequate for inclusion with confirmation of gamma/delta phenotype (especially IHC) being key for inclusion. A clinical tier was also assigned to each case based on group consensus. A composite score was derived by combining pathologic & clinical tiers, with those fitting a pre-determined score threshold included in the primary analysis. Univariate (UVA) associations were derived via Cox model for associations with survival.
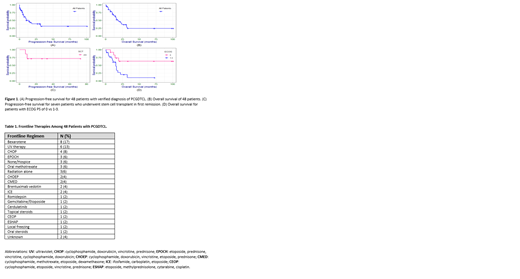
Results: Collectively, all centers submitted a total of 80 cases that were dx & treated locally as PCGDTCL. 48 (60%) cases met pre-defined criteria for inclusion of bona fide dx of PCGTCL. 26 (33%) cases had insufficient composite scores and were grouped in a 2nd tier & 6 cases had incomplete follow-up data and were unsuitable for analysis. The most common reason for placement in the 2nd tier was negativity for gamma/delta IHC or lack of documentation of such testing (n=16). Among the top tier of 48 veritable cases, 32 pts (67%) were male, 39 (81%) white & 4 (8%) black. Median age was 62 years (range 20-88). 19 (40%) pts had B symptoms at dx; ECOG performance status (PS) 0 in 12 pts (25%) & 1-3 in 22 cases (45%) (unknown 29%); anemia was present in 21 pts (44%) & LDH increased in 22 (46%). Bone marrow was involved in only 3 pts (6%) & hemophagocytic syndrome was present at dx in 6 pts (12%). Frontline therapy was heterogeneous (Table 1) with the most common therapies being bexarotene alone in 8 pts; UV therapy in 6 pts; and CHOP in 4 pts. Furthermore, there was inclusion of etoposide in 12 pts (25%), anthracyclines in 9 (19%) & platinum agents in 3 pts (6%). The overall response to 1st line therapy was 40% (19% complete response) with stable disease in 10%, progression in 35% & unknown in 15%. Seven pts (15%) received consolidative stem cell transplantation (SCT), which was allogeneic in all but 1 case. The 2-year PFS for the 48 bona fide pts was 39% (95% CI 0.26-0.59) (Fig 1A) & 2-year OS was 36% (95% CI 0.23-.56) (Fig 1B). The 26 cases in the 2nd tier had overall similar 2-year PFS of 41% (95% CI 0.15-67) and OS of 37% (95% CI 0.22-0.62). In terms of impact of therapy, use of consolidative SCT in 1st remission was associated with improved survival (P=0.02) (Fig 1C). No other therapeutic variable had significance. In UVA for baseline factors, PS (P=0.006) (Fig 1D) and increased vs. normal LDH (P=0.05) were significantly associated with OS. Median OS for pts with normal LDH was 25 months vs 12 months with increased LDH. Median OS for pts with ECOG PS 0 was not reached vs approximately 14 months for ECOG PS 1-3.
Conclusions: To the best of our knowledge, this series represents one of the largest reported to date of PCGDTCL. Accurate diagnosis and classification of PCGDTCL need ongoing analysis and delineation. Using strict criteria, only 60% of cases across 10 academic centers were confirmed as bona fide PCGDTCL. Analysis of these pts treated in the modern era demonstrated modest survival. In addition, we identified several prognostic factors, in particular LDH and ECOG PS, associated with patient outcome. Furthermore, the incorporation of allogeneic SCT in 1st remission may contribute to improved long-term survival. Enhanced treatment options and continued collaboration are critically needed in this rare disease.
Bennani:Adicet Bio: Other: Advisory board; Adicet Bio: Other: Advisory board; Adicet Bio: Other: Advisory board; Kite Pharma: Other: Advisory board; Purdue Pharma: Other: Advisory board; Bristol-Myers Squibb: Research Funding; Purdue Pharma: Other: Advisory board; Seattle Genetics: Other: Advisory board; Bristol-Myers Squibb: Research Funding; Seattle Genetics: Other: Advisory board; Purdue Pharma: Other: Advisory board; Bristol-Myers Squibb: Research Funding; Kite Pharma: Other: Advisory board; Kite Pharma: Other: Advisory board; Seattle Genetics: Other: Advisory board. Landsburg:Takeda: Research Funding; Takeda: Research Funding; Triphase: Research Funding; Seattle Genetics: Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Triphase: Research Funding; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Seattle Genetics: Speakers Bureau; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Haun:Karger, Inc.: Other: Royalties: Textbook. William:Techspert: Consultancy; Guidepoint Global: Consultancy; Defined Health: Consultancy; Celgene Corporation: Consultancy; Kyowa Kirin, Inc.: Consultancy. Mehta-Shah:Kiowa Hakka Kirin: Consultancy; Celgene: Research Funding; Roche/Genentech: Research Funding; Bristol Myers Squibb: Research Funding; Verastem Pharmaceuticals: Research Funding; Innate Pharmaceuticals: Research Funding. Wilcox:Bristol-Myers Squibb: Research Funding; Millenium/Takeda: Research Funding; CTI Biopharma: Research Funding; Incyte: Research Funding. Feldman:AbbVie: Honoraria, Other: Travel expenses, Speakers Bureau; Seattle Genetics: Consultancy, Honoraria, Other: Travel expenses, Speakers Bureau; Eisai: Research Funding; Kyowa Hakko Kirin: Research Funding; Celgene: Honoraria, Research Funding, Speakers Bureau; Takeda: Honoraria, Speakers Bureau; Pfizer: Research Funding; Portola Pharma: Research Funding; Roche: Research Funding; Trillium: Research Funding; Viracta: Research Funding; Roche: Research Funding; Pharmacyclics: Honoraria, Other: Travel expenses, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; Cell Medica: Research Funding; Amgen: Research Funding; Bayer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Kite Pharma: Honoraria, Other: Travel expenses, Speakers Bureau; Corvus: Research Funding. Evens:Tesaro: Research Funding; Pharmacyclics: Consultancy, Honoraria; Epizyme: Consultancy, Honoraria; Verastem: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria, Research Funding. Horwitz:Affimed: Consultancy; Mundipharma: Consultancy; Forty-Seven: Research Funding; Astex: Consultancy; Aileron: Research Funding; Kyowa Hakko Kirin: Consultancy; Infinity/Verastem: Consultancy, Research Funding; Mundipharma: Consultancy; Seattle Genetics: Consultancy, Research Funding; Trillium: Research Funding; Forty-Seven: Research Funding; Trillium: Research Funding; Portola: Consultancy; Kura: Consultancy; Celgene: Consultancy, Research Funding; Astex: Consultancy; Kyowa Hakko Kirin: Consultancy; Aileron: Research Funding; Portola: Consultancy; Kura: Consultancy; Kura: Consultancy; Miragen: Consultancy; Miragen: Consultancy; Portola: Consultancy; Innate Pharma: Consultancy; Millennium/Takeda: Consultancy, Research Funding; Mundipharma: Consultancy; ADCT Therapeutics: Research Funding; Seattle Genetics: Consultancy, Research Funding; Aileron: Research Funding; Forty-Seven: Research Funding; Miragen: Consultancy; Seattle Genetics: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; ADCT Therapeutics: Research Funding; Celgene: Consultancy, Research Funding; Kyowa Hakko Kirin: Consultancy; Corvus Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; ADCT Therapeutics: Research Funding; Infinity/Verastem: Consultancy, Research Funding; Infinity/Verastem: Consultancy, Research Funding; Corvus Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Innate Pharma: Consultancy; Millennium/Takeda: Consultancy, Research Funding; Affimed: Consultancy; Innate Pharma: Consultancy; Affimed: Consultancy; Astex: Consultancy; Trillium: Research Funding; Corvus Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Corvus Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Forty-Seven: Research Funding; Mundipharma: Consultancy; Astex: Consultancy; Celgene: Consultancy, Research Funding; Innate Pharma: Consultancy; Kura: Consultancy; ADCT Therapeutics: Research Funding; Celgene: Consultancy, Research Funding; Infinity/Verastem: Consultancy, Research Funding; Millennium/Takeda: Consultancy, Research Funding; Miragen: Consultancy; Portola: Consultancy; Aileron: Research Funding; Kyowa Hakko Kirin: Consultancy; Affimed: Consultancy; Trillium: Research Funding; Millennium/Takeda: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal