

Introduction: Historically, outcomes for BL have improved in adults using dose intensive chemotherapy regimens and early CNS prophylaxis. More recent data using a less intensive regimen, DA-EPOCH, have been reported. We analyzed detailed patient (pt) & disease characteristics and treatment patterns across 26 US CCs over a recent 9 year (yr) period and also determined survival rates & prognostication.
Methods: We conducted a large multicenter retrospective study of newly diagnosed (dx) adult BL pts (6/2009 - 6/2018). Dx was established by institutional expert pathology review; all cases were verified for BL based on 2016 WHO criteria (high grade B cell lymphoma, BL like, etc were excluded). Survival rates were estimated by Kaplan-Meier with differences assessed by log rank test. Univariate (UVA) associations were derived via Cox model with variables P ≤0.05 entered stepwise into a multivariate (MVA) model. Using significant factors from the MVA, a prognostic survival model was constructed.
Results: Among N=557 verified BL cases, clinical features included: median age 47 yrs (17-88 yrs; 24% ≥60 yrs); male 76%; HIV+ 22%; ECOG PS 0/1 76%; B symptoms 51%; elevated LDH 78% (3, 5, & 10x elevation: 44%, 29% & 15%, respectively); hemoglobin <10.5 gm/dL 32%; albumin <3.5 30%; bone marrow (BM) involved 35%; non-BM extranodal (EN) in 80%; >1 EN 43%; and 76% stage 3-4 disease (10% stage 1). Additionally, 16% and 3% of pts had baseline leptomeningeal (CSF or cranial nerve palsy) or parenchymal CNS involvement, respectively (see Zayac A et al. ASH 2019 for details). For MYC partner, 68% had t(8;14), 4% light chain, 5% negative FISH (otherwise classic BL) and 23% + break apart probe. HIV+ pts had several clinical differences: CSF+ 23% vs 12% P=0.003; CNS 19% vs 8% P<0.001; ECOG PS 2-4 32% vs 21% P=0.002; BM 64% vs 34% P=0.03; and >1 EN 60% vs 38% P<0.001.
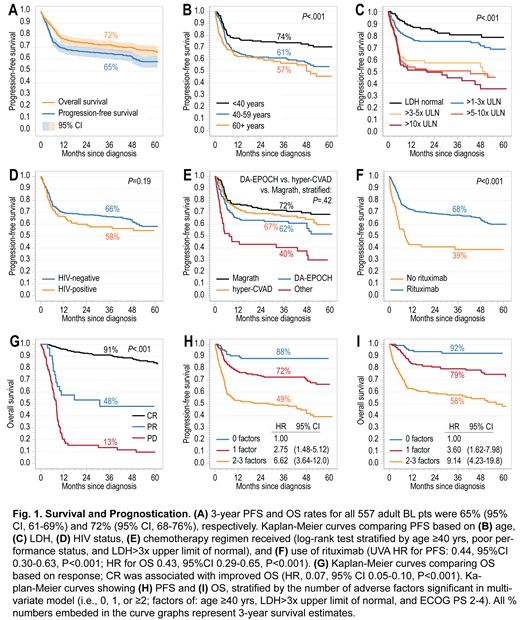
For all pts, 87% had Tx at an academic CC (13% at community CC). Tx regimens were: CODOX-M/IVAC (Magrath) 31%, HyperCVAD/MA 29%, DA-EPOCH 28%, other 10% (mostly CHOP-based & CALGB Tx) & 1% were never treated. 90% of pts received rituximab as part of Tx (69% inpatient (inpt) & 31% outpatient) & 2% had consolidative autologous SCT. Response among all pts were CR 72%, PR 6%, SD 1%, PD 14%, 7% not evaluable. The treatment related mortality (TRM) rate across all pts was 8.9% (HIV+ vs not: 13% vs 8% P=0.09); most common: sepsis 48%, GI bleed/perforation 14% & respiratory failure 12%. TRM by Tx: hyperCVAD/MA 11.5%, EPOCH 6.4%, Magrath 6.3% & other 18.9%. With 39 month median follow-up, 3 year progression-free survival (PFS) and overall survival (OS) were 65% and 72%, respectively (Fig 1A). Among all pts who experienced disease progression, 90% occurred <12 months from dx (4% after 2 yrs). There were 20 cases (4%) of 2nd cancers seen including 7 secondary MDS/AML (median 26 months) & 6 cases of Hodgkin or other NHL (median 54 months).
For prognostication, outcomes were inferior for pts ages ≥40 yrs & LDH >3x normal (Fig 1B/C). Notably, survival rates were not different based on HIV status (Fig 1D) or by the 3 most common Tx regimens (Fig 1E). However, there were important Tx differences based on presence of CNS involvement (see Zayac A et al. ASH 2019). Additionally, use of rituximab was associated with improved PFS & OS (Fig 1F), while outcomes were similar whether rituximab was given inpt vs outpatient (inpt PFS HR 1.25, P=0.19). Furthermore, Tx at an academic CC was associated with improved outcomes, which persisted on MVA (PFS HR 0.54, 95%CI 0.33-0.88 P=0.01; OS HR 0.50, 95%CI 0.29-0.87 P=0.01) & achievement of initial CR was strongly prognostic (Fig 1G). Baseline factors significant on UVA for PFS & OS were: age ≥40 yrs; PS 2-4; LDH >3x; anemia, low albumin; BM involvement; Stage 3-4; CSF+; & >1 EN. On MVA, factors associated with inferior survival were: age ≥40 yrs (PFS HR 1.57, P<0.001; OS HR 1.89, P=0.001); PS 2-4 (PFS HR 1.57, P=0.002; OS HR 2.16, P<0.001); & LDH >3x (PFS HR 2.28, P<0.0001; OS HR 1.96, P<0.0001). Collectively, these factors yielded a BL survival model (Fig 1H/I).
Conclusions: Outcomes for adult BL in this contemporary, large, multicenter RW analysis appear inferior to smaller published series. Interestingly, despite increased adverse prognostic factors, survival rates appeared similar in HIV+ pts. In addition, use of rituximab, achievement of initial CR, and Tx at an academic CC were associated with improved survival. Finally, a novel BL-specific survival model identified pts with markedly divergent outcomes.
Evens:Seattle Genetics: Consultancy, Honoraria, Research Funding; Epizyme: Consultancy, Honoraria; Pharmacyclics: Consultancy, Honoraria; Tesaro: Research Funding; Verastem: Consultancy, Honoraria. Danilov:Janssen: Consultancy; Seattle Genetics: Consultancy; MEI: Research Funding; Abbvie: Consultancy; Pharmacyclics: Consultancy; Takeda Oncology: Research Funding; Janssen: Consultancy; TG Therapeutics: Consultancy; Curis: Consultancy; Pharmacyclics: Consultancy; Aptose Biosciences: Research Funding; Verastem Oncology: Consultancy, Other: Travel Reimbursement , Research Funding; AstraZeneca: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Bayer Oncology: Consultancy, Research Funding; Celgene: Consultancy; Bristol-Meyers Squibb: Research Funding; MEI: Research Funding; Gilead Sciences: Consultancy, Research Funding; Abbvie: Consultancy; Bristol-Meyers Squibb: Research Funding. Reddy:KITE Pharma: Consultancy; BMS: Consultancy, Research Funding; Celgene: Consultancy; Genentech: Research Funding; Abbvie: Consultancy. Farooq:Celgene: Honoraria; Kite Pharma: Research Funding. Khan:Janssen: Other: Educational Content/Symposium; Abbvie: Membership on an entity's Board of Directors or advisory committees; Bristol Myers: Other: Research Funds; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees. Yazdy:Genentech: Research Funding; Bayer: Honoraria; Abbvie: Consultancy; Octapharma: Consultancy. Karmali:Gilead/Kite; Juno/Celgene: Consultancy, Speakers Bureau; Astrazeneca: Speakers Bureau; Takeda, BMS: Other: Research Funding to Institution. Martin:Janssen: Consultancy; Teneobio: Consultancy; Celgene: Consultancy; Karyopharm: Consultancy; Sandoz: Consultancy; I-MAB: Consultancy. Diefenbach:LAM Therapeutics: Research Funding; Incyte: Research Funding; Genentech: Consultancy, Research Funding; Trillium: Research Funding; Millenium/Takeda: Research Funding; Seattle Genetics: Consultancy, Research Funding; Merck: Consultancy, Research Funding; MEI: Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Denovo: Research Funding. Epperla:Pharmacyclics: Honoraria; Verastem Oncology: Speakers Bureau. Feldman:Eisai: Research Funding; Amgen: Research Funding; Cell Medica: Research Funding; Roche: Research Funding; Corvus: Research Funding; Kyowa Hakko Kirin: Research Funding; Pfizer: Research Funding; Trillium: Research Funding; Viracta: Research Funding; Bayer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Speakers Bureau; Celgene: Honoraria, Research Funding, Speakers Bureau; Seattle Genetics: Consultancy, Honoraria, Other: Travel expenses, Speakers Bureau; AbbVie: Honoraria, Other: Travel expenses, Speakers Bureau; Pharmacyclics: Honoraria, Other: Travel expenses, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; Kite Pharma: Honoraria, Other: Travel expenses, Speakers Bureau; Portola Pharma: Research Funding; Roche: Research Funding. Lossos:Janssen Scientific: Membership on an entity's Board of Directors or advisory committees; NIH: Research Funding; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees. Naik:Celgene: Other: Advisory board. Kamdar:Celgene: Consultancy; AstraZeneca: Consultancy; Seattle Genetics: Speakers Bureau; University of Colorado: Employment; Pharmacyclics: Consultancy. Portell:AbbVie: Research Funding; Pharmacyclics: Consultancy; Janssen: Consultancy; Genentech: Consultancy, Research Funding; Bayer: Consultancy; BeiGene: Consultancy, Research Funding; Kite: Consultancy, Research Funding; Acerta/AstraZeneca: Research Funding; TG Therapeutics: Research Funding; Xencor: Research Funding; Roche/Genentech: Research Funding; Infinity: Research Funding; Amgen: Consultancy. Olszewski:Spectrum Pharmaceuticals: Research Funding; TG Therapeutics: Research Funding; Genentech: Research Funding; Adaptive Biotechnologies: Research Funding. Alderuccio:Agios: Other: Immediate family member; Puma Biotechnology: Other: Immediate family member; Foundation Medicine: Other: Immediate family member; Targeted Oncology: Honoraria; Inovio Pharmaceuticals: Other: Immediate family member; OncLive: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal