

Background: Immune thrombocytopenia (ITP) is the most common cause of acquired immune platelet destruction in children. Clinical symptoms range from asymptomatic to significant and even life-threatening bleeding, fatigue, and reduced health-related quality of life. About 75% of affected children experience spontaneous remission, with the remainder developing chronic ITP. Our clinical observations suggest a decreased prevalence of ITP among Black children, although no available studies have evaluated racial or ethnic predisposition to ITP or to chronic disease. We hypothesized that biological differences in Black children alter the prevalence of ITP, relative to the general population, and may affect disease course.
Methods: A retrospective analysis evaluating race and ethnicity of all children with ITP treated at Texas Children's Hospital (TCH, Houston, TX) from January 2015-July 2019 was performed, and compared to both the Houston metropolitan area and the TCH Cancer Center 2018 race and ethnicity data. Of the 699 unique patients, race and ethnicity data were unavailable for 24, and 2 patients were excluded (1 with leukemia, 1 with bone marrow failure). The remaining patients were categorized as (1) White, non-Hispanic; (2) Black, non-Hispanic; (3) Hispanic; and (4) Other. Hispanic patients included those who self-identified as (1) White, Hispanic; (2) Black, Hispanic; (3) Asian, Hispanic; (4) Multi-race, Hispanic; and (5) Unknown race, Hispanic. Demographic data was then collected in a second ITP population derived from the Children's Hospital of Philadelphia (CHOP, Philadelphia, PA) and the surrounding metropolitan area.
To match the distribution reported in the Houston metro area data, a comparison was conducted focusing on the proportion of Black non-Hispanic patients in each cohort. A chi-squared test with Yates correction was utilized to compare nonparametric categorical data using GraphPad Prism version 8.0.1 for Windows, GraphPad Software, San Diego, California, USA. A p-value of <0.05 was statistically significant.
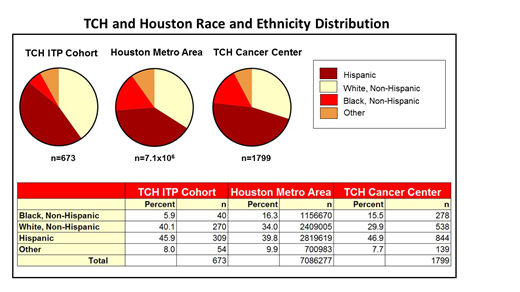
Results: At TCH, there were 673 evaluable ITP patients. Classifying by race only, 42 were Black (6.2%), 564 White (83.8%), and 67 Other (Asian, Mixed Race, Native American, 9.9%). There was a significantly smaller percentage of ITP patients identified as Black, non-Hispanic (n= 40, 5.9%) relative to both the Texas Children's Cancer Center (16% Black, non-Hispanic) and the Houston metropolitan area populations (16% Black, non-Hispanic, p<0.0001). These data are significant given that Texas Children's Hospital sees the majority of children in the Houston metropolitan area, and the demographic data for the Cancer Center accurately reflect the Houston population (see Table). Black, non-Hispanic patients with ITP were more likely to have chronic disease (40% chronic, n=16) than the expected 20-25% in the overall pediatric ITP population. Many of the patients described as Black, non-Hispanic had secondary ITP (20.0%, n=8), most commonly due to systemic lupus erythematosus (SLE), a condition more common amongst Black patients. These findings were consistent at CHOP, with 7% of the 311 included patients classified as Black (n=22), 76% White (n=236) and 17% Other (n=54 including Asian, Middle Eastern, Mixed Race and Native American/Pacific Islander). Again, these proportions are in contrast to the general CHOP patient population (22% Black, 55.5% White and 22.5% other) and the Philadelphia metro population (42.5% Black, 41.5% White, 16% Other). The frequency of chronic ITP was also increased in Black patients in the CHOP cohort (39%, n=7).
Conclusions: This analysis suggests a significant difference in the prevalence of ITP by race in children at two large tertiary care centers in the US. We found that Black children were less likely to develop ITP but those who did were more likely to develop chronic disease relative to other races. Race and ethnicity data at both institutions more closely matched their surrounding metropolitan areas, suggesting the observed differences are not due to care or access barriers. These findings support the possibility that damaging genetic variants, altered gene expression and/or other biological differences in immune response may lead to increased risk of ITP in White children, or protective factors result in reduced prevalence of ITP in Black children. Further research to explore these differences is ongoing.
Lambert:CSL Behring: Consultancy; Amgen: Consultancy, Other; Bayer: Other: Ad boards; Novartis: Other: Ad boards, Research Funding; Shionogi: Consultancy; Kedrion: Consultancy; Sysmex: Consultancy; AstraZeneca: Research Funding; PDSA: Research Funding. Despotovic:Dova: Honoraria; Novartis: Research Funding; Amgen: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal