


Introduction: The WHO 2016 AML-MRC designation applies to AML patients (pts) with: (1) a history of myelodysplastic syndrome (MDS) or MDS/myeloproliferative neoplasm, (2) a MDS-related cytogenetic abnormality, or (3) multilineage dysplasia in >50% of ≥2 cell lineages in the absence of NPM1 or biallelic CEBPA mutations. Pts with AML-MRC typically have a poor prognosis with a low complete remission (CR) rate and short overall survival (OS) after induction chemotherapy. CPX-351 (Vyxeos®; daunorubicin and cytarabine liposome for injection) is a dual-drug liposomal encapsulation of cytarabine [C] and daunorubicin [D] at a synergistic ratio. A large randomized, open-label, multicenter, phase 3 study (NCT01696084) in older pts with newly diagnosed, high-risk/secondary AML found that treatment with CPX-351 significantly improved median OS (9.56 vs 5.95 months; hazard ratio [HR] = 0.69; 1-sided P = 0.003) vs conventional 7+3, with a safety profile comparable to that of 7+3. Based on results of this study, CPX-351 was approved by the FDA and EMA for the treatment of adults with newly diagnosed, therapy-related AML or AML-MRC. An exploratory subgroup analysis of the phase 3 study was performed to compare outcomes in pts with AML-MRC who achieved CR or CR with incomplete neutrophil or platelet recovery (CRi).
Methods: Pts aged 60-75 years with newly diagnosed, high-risk/secondary AML were randomized 1:1 to receive 1-2 induction cycles with CPX-351 (100 units/m2 [C 100 mg/m2 +D 44 mg/m2] as a 90-minute infusion on Days 1, 3, and 5 [2nd induction: Days 1 and 3]) or 7+3 (C 100 mg/m2/day continuously for 7 days [2nd induction: 5 days] + D 60 mg/m2 on Days 1-3 [2nd induction: Days 1-2]). Pts achieving CR or CRi could receive up to 2 consolidation cycles with CPX-351 (65 units/m2 [C 65 mg/m2 + D 29 mg/m2] on Days 1 and 3) or 5+2 (as for 2nd induction). Pts could receive hematopoietic cell transplantation (HCT) at the treating physician's discretion. This exploratory analysis compared outcomes for CPX-351 vs 7+3 in pts who met the WHO 2008 AML-MRC criteria and achieved CR+CRi.
Results: Of 309 enrolled pts, 246 (80%) were diagnosed with AML-MRC (123 pts in each arm). Baseline characteristics of pts with AML-MRC who achieved CR+CRi were generally balanced between arms; 31% and 45% of pts in the CPX-351 and 7+3 arms had antecedent MDS with prior hypomethylating agent (HMA) therapy, 24% and 18% had antecedent MDS without prior HMAs, 7% and 8% had antecedent chronic myelomonocytic leukemia, and 39% and 30% had de novo AML with MDS karyotype. More pts with AML-MRC achieved CR+CRi with CPX-351 (59/123 [48%]) vs 7+3 (40/123 [33%]; odds ratio = 1.83 [95% CI: 1.09-3.09]).
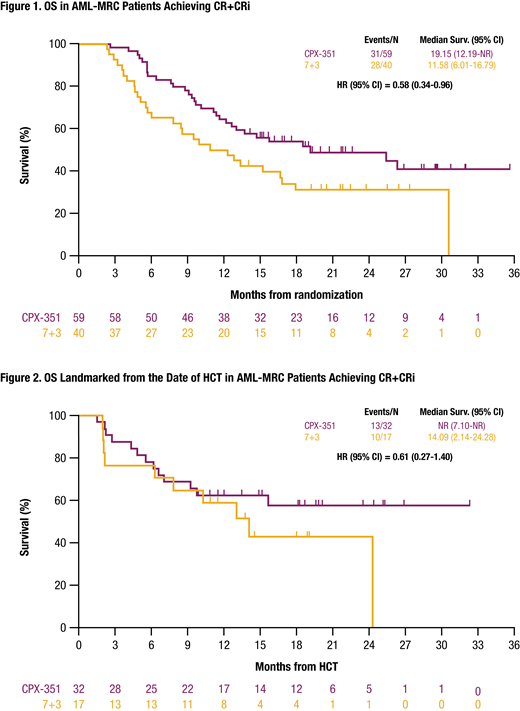
Median OS in pts with AML-MRC who achieved CR+CRi was longer with CPX-351 vs 7+3 (19.15 vs 11.58 months; HR = 0.58 [95% CI: 0.24-0.96]; Figure 1). The HCT rate in AML-MRC pts with CR+CRi was greater with CPX-351 vs 7+3 (54% vs 43%; relative risk = 1.18 [95% CI: 0.79-1.76]), and OS landmarked from the HCT date was longer with CPX-351 (not reached vs 14.09 months; HR = 0.61 [95% CI: 0.27-1.50]; Figure 2). Among pts with de novo AML with MDS karyotype, median OS was 25.43 vs 14.03 months and the HCT rates were 57% vs 50% with CPX-351 and 7+3, respectively, while in pts with antecedent MDS, median OS was 18.53 vs 10.87 months and the HCT rates were 53% vs 44% with CPX-351 and 7+3, respectively.
The most common treatment-emergent adverse events (TEAEs) in pts with AML-MRC who achieved CR+CRi were febrile neutropenia (CPX-351: 78%; 7+3: 80%), constipation (58%; 55%), nausea (53%; 53%), peripheral edema (49%; 65%), fatigue (47%; 50%), and diarrhea (37%; 78%). A cardiac TEAE was experienced by 29 (49%) pts with CPX-351 and 20 (50%) pts with 7+3; the most common events were tachycardia (20%; 18%) and atrial fibrillation (7%; 18%). The most common serious TEAEs were febrile neutropenia (CPX-351: 10%; 7+3: 13%) and ejection fraction decreased (8%; 10%). One pt in each arm discontinued treatment due to a TEAE. There was no early mortality by Day 60 in either arm. CPX-351 was associated with a longer median time to recovery of neutrophils to ≥500/μL (35 vs 29 days) and platelets to ≥50,000/μL (37 vs 28 days) vs 7+3 in pts who received 1 induction cycle.
Conclusions: CPX-351 improved median OS overall and OS landmarked from the date of HCT vs 7+3 chemotherapy in the subgroup of AML-MRC pts who achieved CR+CRi. The safety profile for CPX-351 in this subgroup was consistent with the overall study population and the known safety profile of 7+3.
Ryan:AbbVie: Equity Ownership; University of Rochester: Patents & Royalties. Ritchie:AStella, Bristol-Myers Squibb, Novartis, NS Pharma, Pfizer: Research Funding; Celgene, Novartis: Other: travel support; Jazz Pharmaceuticals: Research Funding; Celgene: Other: Advisory board; Pfizer: Other: Advisory board, travel support; agios: Other: Advisory board; Tolero: Other: Advisory board; Genentech: Other: Advisory board; Celgene, Incyte, Novartis, Pfizer: Consultancy; Ariad, Celgene, Incyte, Novartis: Speakers Bureau. Strickland:Kite: Consultancy; Astellas Pharma: Consultancy; Sunesis Pharmaceuticals: Research Funding; AbbVie: Consultancy; Pfizer: Consultancy; Jazz: Consultancy. Stone:Novartis, Agios, Arog: Research Funding; Argenx, Celgene, Takeda Oncology: Other: Data and Safety Monitoring Board/Committee: ; AbbVie, Actinium, Agios, Argenx, Arog, Astellas, AstraZeneca, Biolinerx, Celgene, Cornerstone Biopharma, Fujifilm, Jazz Pharmaceuticals, Amgen, Ono, Orsenix, Otsuka, Merck, Novartis, Pfizer, Sumitomo, Trovagene: Consultancy. Schiller:Constellation Pharmaceutical: Research Funding; Astellas: Research Funding; Biomed Valley Discoveries: Research Funding; Bristol Myer Squibb: Research Funding; Amgen: Other, Research Funding; Agios: Research Funding, Speakers Bureau; Daiichi Sankyo: Research Funding; Eli Lilly and Company: Research Funding; FujiFilm: Research Funding; Genzyme: Research Funding; Gilead: Research Funding; Incyte: Research Funding; J&J: Research Funding; Jazz Pharmaceuticals: Honoraria, Research Funding; Karyopharm: Research Funding; Novartis: Research Funding; Onconova: Research Funding; Pfizer Pharmaceuticals: Equity Ownership, Research Funding; Sangamo Therapeutics: Research Funding; Celgene: Research Funding, Speakers Bureau. Wieduwilt:Amgen, Leadiant, Merck, Servier: Research Funding; Reata Pharmaceuticals: Equity Ownership; Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees. Ryan:Jazz Pharmaceuticals: Employment, Equity Ownership. Faderl:Jazz Pharmaceutics: Employment, Equity Ownership. Cortes:Takeda: Consultancy, Research Funding; Merus: Consultancy, Honoraria, Research Funding; Biopath Holdings: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Research Funding; Astellas Pharma: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Immunogen: Consultancy, Honoraria, Research Funding; BiolineRx: Consultancy; Sun Pharma: Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal