

Background: Comorbidities and other patient factors in multiple myeloma (MM) can affect treatment decision making. While chemotherapy selection for MM in Medicare populations is different between blacks and non-blacks, including decreased use of bortezomib (BTZ) and hematopoietic cell transplant (HCT), data from the Veterans Health Administration (VHA) has previously shown no difference in selection. Little is known about the interaction between race and comorbidities on treatment of MM. In order to understand possible effects of race and comorbidities in management of MM, we studied initial treatment patterns in a nationwide population of United States veterans cared for in the VHA.
Methods: Patients with MM were identified by the VHA Central Cancer Registry between July 1, 2006 and December 31, 2013 and followed through December 31, 2014. Age, sex, race, body mass index (BMI), Charlson comorbidities index (CCI) from ICD9 codes prior to diagnosis, hemoglobin (hgb), albumin, renal function via MDRD equation (GFR), and HCT were collected. Treatment data was collected from pharmacy records, all patients had to receive treatment within 6 months of diagnosis. T-test and chi-square analyses were used to compare continuous and categorical variables respectively. Logistic regression modeling was used to assess the association between receipt of MM treatments, race, and comorbidities. Cox proportional hazards regression modeling was used to assess the association between race and overall survival at five years while controlling for known prognostic factors. The study was approved the Saint Louis VA Medical Center institutional review board.
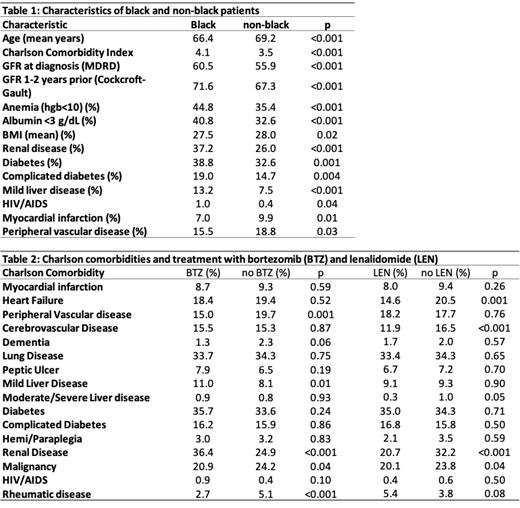
Results: 2940 patients were identified with MM, of which 884 (30.1%) were black. Black patients were younger with increased mean CCI, lower mean BMI, higher GFR at diagnosis and 1-2 years prior to diagnosis, with higher rates of anemia and albumin below 3 g/dL compared to non-black patients (Table 1). Black patients had significantly higher rates of renal disease (37.2% vs. 26.0%, p<0.001), diabetes (38.8% vs. 32.6%, p=0.001), complicated diabetes (19.0% vs. 14.7%, p=0.001), mild liver disease (13.2% vs. 7.5%, p<0.001) based on CCI calculated from ICD codes. Black patients were less likely to be treated with lenalidomide (LEN) in their initial regimen (21.3% vs. 26.1%, p=0.03) or have HCT in one year (7.5% vs. 10.6%, p=0.01), more likely to be treated with BTZ (43.8% vs. 37.1%, p=0.001), and there was no difference in treatment with THAL (20.9 vs 20.6%, p=0.85) or in the number of therapies in the initial regimen (2.0 vs. 2.0, p=0.62). After adjusting for GFR and CCI, black race remained associated with decreased use of LEN (Odds Ratio 0.76, 95% CI 0.62-0.92). After controlling for age, race, CCI, BMI, anemia, GFR, albumin, HCT within 5 years, patients had improved survival at 5 years when initially treated with LEN (HR 0.71, 95% CI 0.61-0.82) and thalidomide (THAL) (HR 0.85, 95% CI 0.74-0.98), but not with BOR (HR 0.92, 95% CI 0.82-1.05). After adjusting for age, CCI, BMI, anemia, GFR, albumin, HCT within 1 year, LEN, BTZ, and THAL as initial treatment, black patients had improved survival (HR 0.79, 95% CI 0.71-0.89) compared to non-blacks at 5 years.
Conclusions: Disparities in treatment exist for black patients with MM in the VHA, despite improved mortality compared to non-blacks. Black patients in the VHA are younger, with higher CCI, particularly renal disease, diabetes and liver disease. Interestingly, actual measurements of GFR at diagnosis and 1 year prior are higher in blacks which is contrary to the increased rate of renal disease assessed by ICD9 codes. Clinicians may misperceive renal function due to higher baseline creatinine levels in blacks, which could lead to attribution of renal comorbidity and reduced use of LEN in black patients. Further evaluation of the interaction between race, comorbidities, and treatment is warranted.
Schoen:Pharmacyclics: Research Funding. Carson:Flatiron Health, Inc., which is an independent subsidiary of the Roche Group: Employment, Research Funding; Roche: Equity Ownership. Sanfilippo:Bristol-Myers Squibb: Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees; Bayer: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Other: Travel Expenses; NHLBI: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal