

Importance: Plasma is frequently transfused to patients who are bleeding or require an invasive procedure and have a deficiency of coagulation factors. Despite published guidelines delineating optimal plasma use, two recent audits have suggested that over 50% of the plasma transfused is unnecessary. Inappropriate utilization of plasma has numerous adverse consequences for the recipient, as well as the health care system.
Objective: To determine the proportion of inappropriate plasma use with a multicenter electronic data audit and identify focused areas for intervention to reduce inappropriate use.
Setting: 3 tertiary care academic sites across Ontario, Canada: Hamilton Health Sciences Centre (Hamilton, Ontario), Sunnybrook Health Sciences Centre (Toronto, Ontario), London Health Sciences Centre (London, Ontario).
Participants: All adult inpatients receiving plasma during the time period January 1, 2017 and December 31, 2017.
Design: Four areas of inappropriate plasma use in adult patients were defined: (1) patients with a normal INR <1.5 and who were not actively bleeding or moderate bleeding only (1 unit RBC transfused within 24 hours before or after plasma transfusion or 20 g/L drop in hemoglobin); (2) elevated INR >1.5, without active bleeding or procedures in 6 hours after plasma transfusion (1 calendar day when time of procedure was not available); (3) no INR drawn before or after plasma infusion; (4) inappropriate non-therapeutic plasma dose of plasma (≤ 2 units) .
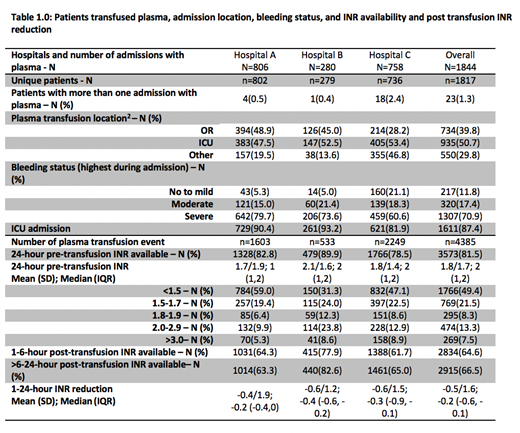
Results: A total 4,385 plasma transfusion events occurred in 1,844 inpatient admissions. Appropriate indication and dosing was found in 813 (18.5%) of the events. Inappropriate compliance occurred in 3,572 (81.5%) of the events: 608 (13.9%) events occurred in the pre-specified criteria (1-3) above; inappropriate dosing alone occurred in 1,583 (36.1%) events; and, a combination of inappropriate dosing in addition to any 1-3 pre-defined categories occurred in 1,381 (31.5%) transfusion events. Patients transfused with a documented INR (81.5%) in the 24 hours preceding plasma transfusion had a mean INR value 1.8+1.7 (INR + SD). The mean overall reduction after 1-24 hours of plasma transfusion was -0.5+1.6 .
Conclusions and Relevance: A significant amount of plasma is transfused inappropriately, leading to potential patient harm, significant unnecessary costs, and diversion of plasma away from fractionation impacting the supply of intravenous immunoglobulin. This study will inform a large quality improvement study aimed at reducing unnecessary plasma transfusion.
Heddle:Novartis: Research Funding. Arnold:Principia: Consultancy; Bristol-Myers Squibb: Research Funding; Novartis: Honoraria, Research Funding; Rigel: Consultancy, Research Funding. Hsia:Amgen: Honoraria; Jansen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal