

Purpose
Although minimal residual disease (MRD) is an established surrogate marker for outcomes following treatment with chemoimmunotherapy, less is known about the value of MRD in chemotherapy-free treatments in the first-line setting. We investigated the prognostic value of MRD detection after a fixed-duration treatment of venetoclax plus obinutuzumab (VenG) with respect to clinical and genetic risk factors and source of material in previously untreated patients (pts) with CLL and coexisting conditions.
Methods
In this multinational, open-label, Phase 3 trial, 432 previously untreated pts with a Cumulative Illness Rating Scale score >6 and/or an estimated creatinine clearance <70 mL/min were randomized 1:1 to receive chlorambucil or venetoclax (216 pts per treatment group) until completion of cycle 12, and in combination with obinutuzumab for the first 6 cycles. The primary endpoint was progression-free survival (PFS), MRD was a secondary endpoint. Peripheral blood (PB) samples for MRD were taken at cycle 7, 9, and 12, and then serially every 3 months. In pts with a treatment response, MRD in bone marrow (BM) was assessed at cycle 9 and 3 months after end of treatment (EOT). MRD was analyzed by quantitative immunoglobulin allele-specific real-time (IGH-ASO)-PCR (cut-off: 10-2 and 10-4) and additionally by next-generation sequencing (NGS, Adaptive Clonoseq assay, cut-off: 10-4, 10-5 and 10-6). Outcome was analyzed according to known MRD risk groups i.e. detectable (≥10-4) and undetectable (<10-4) as well as to known clinical and biological risk factors. Landmark PFS and time to MRD re-detection from EOT were analyzed using Kaplan-Meier methodology. Apart from re-detection to MRD level ≥10-4, pts with a competing event (including progression of disease, relapse, new CLL therapy, and death) also counted towards the MRD re-detection events total.
Results
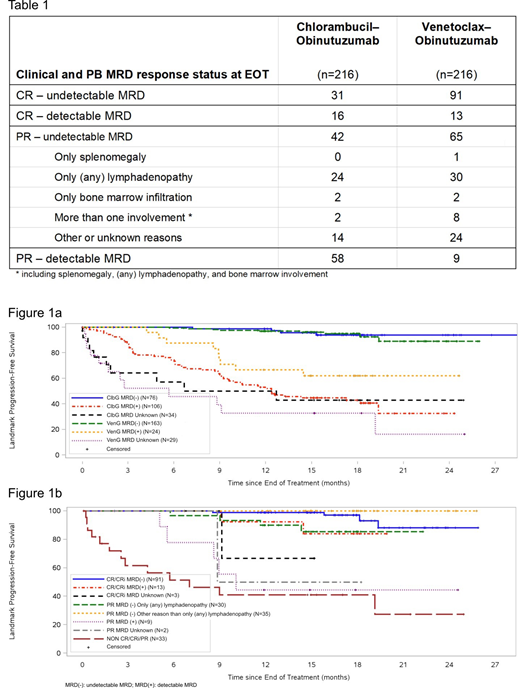
On the basis of the intention-to-treat population (i.e. for the full trial population and irrespective of sample availability), VenG achieved higher rates of undetectable MRD at EOT compared with chlorambucil and obinutuzumab (ClbG) (PB: 75.5% vs. 35.2%, BM: 56.9% vs. 17.1%). In contrast, detectable MRD in PB was found in 19 (8.8%) VenG pts and 103 (47.7%) ClbG pts. Of these, 11 (5.1%) VenG vs. 47 (21.8%) ClbG pts had intermediate MRD at ≥10-4-<10-2 and 8 (3.7%) vs. 56 (25.9%) pts had high positive MRD at cut-off 10-2. Of the 19 VenG pts with detectable MRD, 64.3% had unmutated IGHV, 22.2% had a TP53 disruption and 17.6% had a complex karyotype. In pts with undetectable MRD in PB, the rate of complete response at EOT was higher with VenG than with ClbG (55.8% vs. 40.8%, Table 1). Achieving undetectable MRD in PB with VenG was associated with a high proportion of patients with corresponding BM clearance of 74.8% with only 4.9% of pts being BM MRD-detectable. In addition, depth of MRD response measured by NGS was more profound in VenG compared to ClbG (<10-5: 67.6% vs. 19.9%, <10-6: 42.1% vs. 6.5%) with undetectable MRD according to both NGS and IGH-ASO-PCR at cut-off 10-4 in 74.5% of pts treated with VenG and an overall concordance between both methods of 95.4%. Considering pts with undetectable MRD in PB at EOT, the time to MRD re-detection was longer with VenG than with ClbG (median 17.7 months and 34 (20.9%) re-detection events with VenG vs. median 7.5 months and 55 (72.4%) re-detection events with ClbG, HR 0.192, 95% CI 0.124-0.296). In landmark analysis from EOT, undetectable MRD correlated with favourable PFS rates at 24 months as compared with detectable MRD: 89.1% vs. 61.9% in VenG and 93.9% vs. 32.6% in ClbG, respectively. Median PFS was not reached in undetectable MRD groups (Figure 1a). Further landmark analysis of PFS by MRD status showed that undetectable MRD translated into improved PFS regardless of the clinical response status at EOT (Figure 1b).
Conclusion
Fixed-duration treatment with VenG achieves unprecedentedly high and sustainable rates of undetectable MRD in patients with previously untreated CLL and coexisting conditions. Findings confirm the prognostic value of MRD assessment at EOT for this chemotherapy-free treatment regimen. Due to high concordance of undetectable MRD in PB and BM in the context of VenG, BM assessments may not be required for these patients.
Fischer:Roche: Other: travel grants; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees. Ritgen:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Membership on an entity's Board of Directors or advisory committees; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support, Research Funding. Al-Sawaf:Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support; Janssen: Membership on an entity's Board of Directors or advisory committees, Other: travel support; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support. Tandon:Roche: Equity Ownership; Roche Products Ltd: Employment. Fink:Janssen: Membership on an entity's Board of Directors or advisory committees; Celgene: Research Funding; Roche: Other: travel grants. Stübig:Hexal: Speakers Bureau. Brüggemann:Amgen, Celgene, Janssen: Honoraria, Speakers Bureau; Amgen, Janssen: Membership on an entity's Board of Directors or advisory committees; affimed, Amgen, Celgene, Regeneron: Research Funding; Amgen, Incyte, PRMA: Consultancy. Jiang:Genentech: Employment, Equity Ownership; F. Hoffman-La Roche: Equity Ownership. Schary:Abbvie: Employment, Equity Ownership. Eichhorst:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; BeiGene: Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead Sciences, Inc.: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; ArQule: Membership on an entity's Board of Directors or advisory committees. Wendtner:MorphoSys: Consultancy, Honoraria, Research Funding; GILEAD Science: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Janssen-CILAG: Consultancy, Honoraria, Research Funding; Novartis: Honoraria, Research Funding; F. Hoffmann-La Roche Ltd: Consultancy, Honoraria, Research Funding; Mundipharma: Honoraria, Research Funding. Tausch:AbbVie: Consultancy, Honoraria, Other: travel support, Speakers Bureau; Roche: Consultancy, Honoraria, Speakers Bureau. Kreuzer:Roche and Abbvie: Honoraria, Other: Expert testimony. Langerak:F. Hoffmann-La Roche Ltd: Research Funding; Gilead: Research Funding, Speakers Bureau; Janssen: Speakers Bureau; Genentech, Inc.: Research Funding. Goede:Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel grants, speaker fees, Speakers Bureau; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: speaker fees, Speakers Bureau; janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel grants, speaker fees, Speakers Bureau. Böttcher:AbbVie: Honoraria, Other: Travel grants, Research Funding; Celgene: Research Funding; Janssen-CILAG: Honoraria, Other: Travel grants, Research Funding; Roche: Honoraria, Research Funding; Genentech: Research Funding; Becton Dickinson: Research Funding; Novartis: Research Funding. Stilgenbauer:AstraZeneca: Consultancy, Honoraria, Research Funding, Speakers Bureau; AbbVie: Consultancy, Honoraria, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Pharmacyclics: Other: Travel support; Gilead: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Novartis: Consultancy, Honoraria, Research Funding, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Hoffmann La-Roche: Consultancy, Honoraria, Research Funding, Speakers Bureau. Hallek:Roche, Gilead Sciences, Inc., Mundipharma, Janssen, Celgene, Pharmacyclics, AbbVie: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal