

Introduction
Elevated serum ferritin (hyperferritinemia, HF) can result from increased iron load, increased inflammation or from liver damage. In the most common forms of hereditary hemochromatosis (HH), elevated ferritin is usually seen with elevated transferrin saturations, [1,2]. In patients with HF but without raised liver iron concentration (LIC, mg/g dry wt [dw]), increased liver fat (hepatic steatosis, HS), either in isolation or as part of a metabolic syndrome, needs to be considered. HS is important to identify as it may progress to chronic liver damage and is potentially reversible with lifestyle interventions. Hepatic fat can now be quantified with magnetic resonance imaging (Hepafat-Scan®)[3]. Here, we evaluate the usefulness of this method in the diagnosis and subsequent management of patients referred with HF.
Methods
A total of 132 patients (median age 48 years, range 21-86 ; female: male ratio 1:2.5) referred for investigation of HF and who underwent estimation of liver iron concentration (LIC) by R2-MRI (FerriScan®) over a four-year period (January 2015 - December 2018) are included in this analysis. Data on patient demographics, presenting serum ferritin (SF) and transferrin saturation were obtained. Genetic testing for C282Y and H63D was also performed. Genetic testing for rarer forms of haemochromatosis was confined to patients with unexplained raised LIC. Patients with iron overload secondary to chronic iron ingestion or blood transfusion were excluded from this analysis.
Results
Patients were subdivided by genetic diagnosis: C282Y homozygote (26, 19.7%), C282Y/H63D (18, 13.6%), H63D homozygote (10, 7.6%), C282Y heterozygote (8, 6.1%), H63D heterozygote (18, 13.6%), autosomal dominant ferroportin disease (4, 3%) and negative HFE gene testing (48, 36.4%). There was no statistical difference between mean presenting SF (p= 0.307) between the different groups. C282Y homozygotes, and those with autosomal ferroportin disease had a significantly higher LIC than others (p<0.001). C282Y homozygotes and compound heterozygotes had a significantly higher transferrin saturation than other groups (p<0.001). SF positively correlated with LIC (p<0.001).
After genetic testing and LIC quantification, 32 patients underwent a HepaFat-Scan®. Median age was 63 years, range 23 - 74 years; female: male ratio 1:3.5. 54.5% had a volumetric liver fat fraction (VLFF) > 5%. 7.4% of patients, who did not undergo Hepafat-Scan®, had HS based on sonographic findings. Patients with definitive evidence of HS as defined by VLFF >5% had mean LIC of 1.36mg/g dw, and a higher mean presenting SF of 926 µg/L than those with HS <5% (NS, p= 0.47). Those with VLFF <5% had a mean presenting SF of 783 mg/ml and mean LIC of 2.2 mg/g dw.
In patients with LIC ≤3mg/g dw (n= 91, mean 1.6), mean presenting SF was 728 mg/ml. 28 of these patients went onto have a Hepafat-Scan®, 16 of which (57.1%) had confirmed steatosis with VLFF >5%. In patients with LIC >3mg/g dw (n= 41, mean LIC 6.9), mean presenting SF was significantly higher at 1056 mg/ml (p=0.021). 4 patients with LIC >3mg/g dw also had a Hepafat-Scan®, with 1 patient having VLFF >5%. Patients with confirmed steatosis were referred for specialist hepatology consultation.
Conclusion
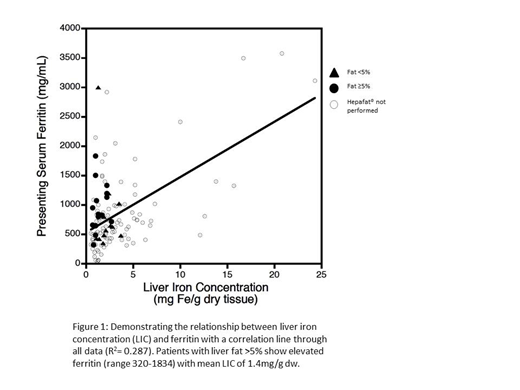
In patients referred for investigation of HF, demonstrable steatosis (VLFF >5%) by Hepafat-Scan® is remarkably high (13.3% of all referred patients and 54% of patients who received Hepafat-Scan®). The Hepafat-Scan® data show that HS is generally confined to patients with low LIC (≤3mg/g dw) (Figure 1) reflecting the selective decision pathway adopted of excluding hepatic siderosis before proceeding to Hepafat-Scan®. SF is significantly higher in non-iron overloaded patients with HS (VLFF >5%) than those without HS (Figure 1). Estimation of HS should be considered in the diagnostic pathway of patients referred for investigation of HF, particularly when LIC values are not found to be meaningfully increased.
References
1. Cullis JO et al. Investigation and management of a raised serum ferritin. British Journal of Haematology 2018; 181:331-340
2. St Pierre TG et al. Noninvasive measurement and imaging of liver iron concentration using proton magnetic resonance. Blood. 2005; 105(2):855-61
3. St Pierre TG et al. Stereological Analysis of Liver Biopsy Histology Sections as a Reference Standard for Validating Non-Invasive Liver Fat Fraction Measurement by MRI. PLoS ONE August 2016; 11(8):e0160789
Eleftheriou:Novartis: Honoraria. Garbowski:Imara: Consultancy; Vifor Pharma: Consultancy. St. Pierre:Resonance Health Ltd: Consultancy, Other: Share ownership. Porter:Agios: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Protagonism: Honoraria; La Jolla: Honoraria; Vifor: Honoraria; Silence therapeutics: Honoraria; Bluebird bio: Consultancy, Honoraria. Drasar:Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal