

Background: ATO was approved by the U.S. Food and Drug Administration in 2000 for treatment of patients with relapsed/refractory APL and in 2018 in combination with all-trans retinoic acid (ATRA) for adults with newly-diagnosed low-risk APL. ATRA and ATO combinations result in long-term remissions in most patients with APL (Lo-Coco et al. NEJM 2013, Burnett et al. Lancet Oncol 2015). However, epidemiologic studies have shown associations between exposure to inorganic arsenic and development of skin, lung, bladder, and potentially liver, kidney, and prostate cancers (IARC 2004). The prescribing information for ATO includes a warning for carcinogenesis, with advice to monitor patients for development of second primary malignancies. Retrospective cohort analyses of second cancers in APL patients treated with ATO have been performed, finding incidence rates of 1-5% (Eghtedar et al. Leuk Lymphoma 2015, Au et al. Leuk Res 2007, Zhu et al. Blood 2016). We sought to perform an exploratory population-based analysis of second cancers in adults with APL treated with ATO compared to those treated with other systemic APL therapies without ATO using the linked Surveillance, Epidemiology, and End Results (SEER)-Medicare database.
Methods: Using SEER-Medicare linked data, we identified APL patients diagnosed from January 1, 2006 to December 31, 2015. Patients whose first SEER cancer diagnosis was APL, who were continuously enrolled in Medicare Parts A, B, & D from the month of their APL diagnosis, and who received treatment with ≥ 1 systemic APL therapy within 1 year of diagnosis were included. Patients were followed from their first month of treatment group-defining APL therapy (ATO or non-ATO containing) until disenrollment from Medicare Parts A, B, or D, end of study period, or death. We determined the cumulative incidence of SEER-confirmed second cancers and overall survival (OS) according to whether patients were treated with or without ATO using the Kaplan-Meier method. We used a multivariate Cox proportional hazards model to estimate the hazard ratios (HR) and 95% confidence intervals (CI) of cumulative incidence of second cancers and OS adjusted for relevant covariates of age, sex, and year of diagnosis.
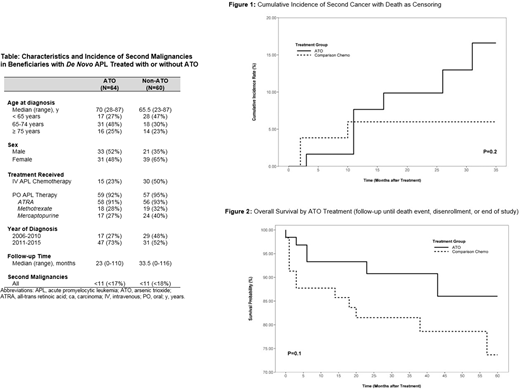
Results: We identified 1,442 APL cases, with 1,179 having APL as their first cancer diagnosis, of which 246 were enrolled in Medicare Parts A, B, and D. Of these, 64 received ATO and 60 received systemic APL therapy without ATO within 1 year of diagnosis. Characteristics, follow-up, and second malignancies for these cohorts are presented in the Table. Absolute incidence rates of second cancer were 3.4 per 1000 person-months compared to 1.4 per 1000 person-months in patients treated with and without ATO, respectively, and cumulative incidence rates at 24 months were 9.9% and 6.0%, respectively (p=0.20) (Figure 1). Mortality rates were 1.9 per 1000 person-months compared to 5.1 per 1000 person-months in patients treated with and without ATO, respectively, and OS rates at 24 months were 90.8% and 81.5%, respectively (p=0.10) (Figure 2). After adjusting for relevant covariates, HR for cumulative incidence of second malignancies in patients treated with ATO was 1.27 (95% CI 0.29-5.49; p=0.75) and for OS was 0.46 (95% CI 0.16-1.29; p=0.14) compared to APL therapy without ATO.
Conclusions: This exploratory analysis revealed a high incidence of second malignancies in APL patients treated with ATO, although the risk was not significantly increased compared to patients who received other APL therapies. Most second malignancies following ATO were solid tumors, in line with prior epidemiologic studies of inorganic arsenic exposures. Despite the occurrence of second malignancies, there was a tendency towards longer OS in patients treated with ATO. Given the small sample size, short follow-up, potential selection and immortal time bias, and unaccounted for differences between comparator groups, firm conclusions cannot be inferred. However, the nearly 10% cumulative incidence of second malignancies at 24 months follow-up in Medicare patients with APL treated with ATO suggests the need for close monitoring for second malignancies following ATO therapy. Further prospective research into second malignancies following ATO is needed.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal