

Background: MM is associated with significant morbidity even at the time of presentation and there is ample data to support that MM treatment improves overall survival (OS) as well as quality of life (QoL) due to effective symptom control. Patient refusal to recommended cancer treatment is not common in clinical practice but has been reported in certain cancers. There is no data on characteristics of MM patients who refuse treatment despite physician recommendation and outcomes of such patients.
Methods: We used the National Cancer Database (NCDB) from 2004-2015 to extract data on adult MM patients who refused any systemic therapy as part of their initial care despite physician recommendation. Information on patient age, gender, race/ethnicity, education, year of diagnosis, income, geographical location, comorbidities, systemic treatment, survival time and vital status was obtained. Average annual percent change (AAPC) and average percent change (APC) were calculated to analyze the trends, and periods with similar APC were compared for statistically significant changes by applying join point regression. Multivariate models were employed to identify factors predicting refusal to therapy and to assess its impact on OS.
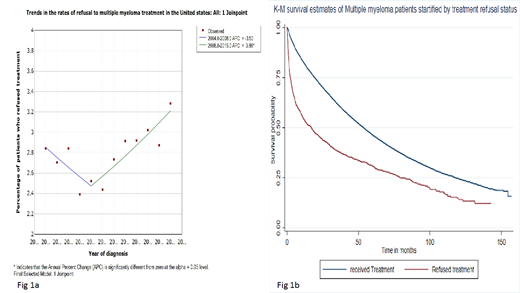
Results: Of 75,734 eligible patients who were recommended treatment for MM (chemotherapy and or immunotherapy), 2138 (2.8%) patients did not receive any treatment due to refusal. Significantly higher number of females, patients in older age groups (age groups 60-79 and ³ 80 years), Medicare recipients and with ≥2 comorbidities refused treatment recommendation. On multivariate analysis, advanced age groups 60-79 years (OR = 1.47; 95% CI 1.27-1.31 p<0.001) and ³80 years (OR = 5.02; 95% CI 4.23-5.96, p<0.001), female gender (OR =1.16 ; 95% CI 1.05-1.27, p<0.001), patients with certain primary payor types including Medicaid (OR = 1.59; 95% CI 1.28-1.98, p<0.001), Medicare (OR = 1.63; 95% CI 1.43-1.87, p<0.001) and uninsured (OR = 1.81; 95% CI 1.38-2.38, p<0.001), and presence of ³2 comorbidities (OR = 1.39; 95% CI 1.2-1.61, p<0.001) were the independent factors associated with higher likelihood of refusing treatment. Whereas being seen at academic research programs (OR = 0.7; 95% CI 0.6-0.8, p<0.001), higher education (OR =0.81 ; 95% CI 0.67-0.98, p=0.03), geographical location (Midwest OR =0.87 ; 95% CI 0.76-0.99, p=0.04), longer distance to facility being at 3rd quartile (10.1-26.2 miles: OR =0.78 ; 95% CI 0.68-0.89, p<0.001) or 4th quartile (>26.2 miles: OR = 0.59; 95% CI 0.51-0.68, p<0.001) were associated with lower likelihood of refusing treatment. The overall rate of refusing treatment by MM patients was quite stable during 2004-2015 with an AAPC of 1.1 (95% CI -1.1-3.3 p=0.3). However, on fitting scatter plot into Joinpoint regression model, a concerning trend in the more recent years was noted. While the rate of refusing recommended treatment decreased during 2004-2008, a rising trend was observed during the period 2008-2015 with an APC of 3.8 (95% CI 1.3-6.4, p≤0.001) (Fig 1a). Patients who were recommended treatment but refused had significantly worse survival than those who received treatment (median survival 17.7 vs 52.9 months, Cox hazard ratio 1.21; CI 1.17-1.24, p<0.001) (Fig 1b).
Conclusions: The percentage of MM patients refusing any systemic treatment as a part of their initial care despite physician recommendation appears to be increasing in recent years and this needs to be systematically addressed. Disparities in refusal to recommended treatment are independently associated with several variables including age, gender, comorbidities, geographical location, facility and insurance type. These need to be addressed urgently since there are several effective and well-tolerated anti-MM treatments which can potentially benefit patients in case the initial socioeconomic, clinical and psychosocial barriers are overcome.
Chanan-Khan:Xencor: Research Funding; Pharmacyclics: Research Funding; Merck: Research Funding; Jansen: Research Funding; Mayo Clinic: Employment; Ascentage: Research Funding; Millennium: Research Funding; AbbVie: Research Funding. Ailawadhi:Pharmacyclics: Research Funding; Celgene: Consultancy; Amgen: Consultancy, Research Funding; Cellectar: Research Funding; Janssen: Consultancy, Research Funding; Takeda: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal