

Introduction: There is limited contemporary evidence on clinical outcomes and healthcare use in sickle-cell disease (SCD) patients enrolled in US Medicaid. We aimed to provide contemporary estimates for rates of vaso-occlusive crises (VOC), mortality, and healthcare resource utilization (HRU) in SCD patients enrolled in US Medicaid.
Methods: We conducted a cohort study using nationwide Medicaid insurance claims data (2000-2013). Patients were included based on ≥1 inpatient or ≥2 outpatient HbSS SCD diagnosis claims after 365 days continuous enrollment in Medicaid (or continuous eligibility since birth if age at diagnosis is <1 year). Patients were followed until Medicaid disenrollment, death, bone marrow transplant, or end of data availability (December 31, 2013). Outcomes included frequency of VOCs, event rates of HRU including emergency department (ED) visits, hospitalizations, outpatient visits, and blood transfusions, and all-cause mortality during the follow-up period. All outcomes were reported as annualized event rates (with 95% confidence intervals). VOCs were stratified by age-group (<1, 2-6, 7-12, 13-18, 19-35, 35+ years), VOCs at baseline (<2, 2-4, >=5), race (African American or not), and sex. The impact of VOCs on the risk of mortality was analyzed using an extended multivariable Cox model with VOCs modeled as time-varying and updated annually.
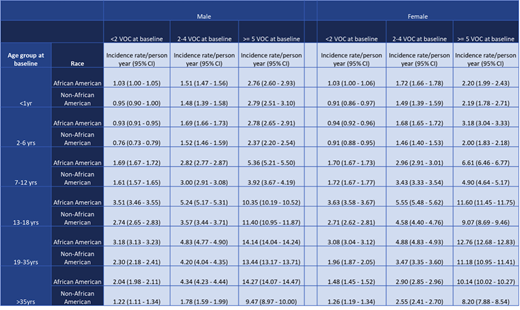
Results: A total of 44,033 SCD patients were included in the analysis; 47% were female, 82% were African American, and a mean (SD) age of 15.7 (13.6). The average VOC rate was 3.71 (95% CI: 3.70-3.72) VOCs per person-year over an average follow-up period of 4.3 years. The rate of VOCs was substantially higher among patients aged 19-35 years and those with a higher VOC frequency at baseline (Table 1). Overall, the event rates (95%CI) per person year for other HRU outcomes were: 2.97 (2.97-2.98) ED visits, 2.39 (2.38-2.40) hospitalizations, 5.80 (5.79-5.81) outpatient visits, and 0.91 (95%CI: 0.90-0.91) blood transfusions. The mortality rate was 1.13 (95%CI: 1.08-1.17) events per 100 person-years overall, with the highest rate being 4.91 (95%CI: 4.58-5.25) events per 100 person-years among patients ≥ 35 years of age. Higher VOC burden in the preceding year was associated with an increased risk mortality: 2-4 VOC vs. 0 or 1 VOC: Hazard Ratio (HR)=1.36 (95%CI: 1.21-1.52); ≥ 5 VOC: HR= 1.56 (95%CI: 1.39-1.75).
Conclusion: The burden of SCD in US Medicaid enrollees is substantial, especially during early adulthood, with markedly high rates of VOCs, mortality, and healthcare utilization. A higher VOC rate in the preceding year was associated with an increased risk of mortality suggesting a need for careful management of SCD patients with higher VOC burden.
Table 1. Annualized rates of vaso-occlusive crises (VOC) among sickle cell disease patients enrolled in Medicaid. VOC, vaso-occlusive crises; CI, confidence interval.
Desai:Merck: Research Funding; Bayer: Research Funding. Globe:Vertex Pharmaceuticals Incorporated: Employment. McKerracher:CRISPR Therapeutics: Employment. Mutebi:Vertex Pharmaceuticals Incorporated: Employment. Bohn:Bohn Epidemiology: Equity Ownership; Vertex Pharmaceuticals Inc: Consultancy. Achebe:Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees; Pharmacosmos: Membership on an entity's Board of Directors or advisory committees; Fulcrum Therapeutics: Membership on an entity's Board of Directors or advisory committees; Bluebird Bio: Membership on an entity's Board of Directors or advisory committees. Schneeweiss:Genentech: Research Funding; Boehringer Ingelheim: Research Funding; Aetion, Inc.: Consultancy, Equity Ownership; Whiscon LLC: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal