

Introduction
Several studies have shown that the induction of antibodies by natural exposure to various AAV serotypes can compromise the subsequent use of AAV as a gene therapy vector, limiting patient eligibility for AAV-delivered therapeutics. The implications of pre-existing antibodies to AAV serotypes are very different: Levels of anti-AAV2 or anti-AAV8 neutralizing antibodies (NABs) as low as 5 have been related to a decrease or even total impairment of AAV liver transduction after systemic delivery in humans. However, successful gene transfer has been reported in patients with anti-AAV5 NABs titers up to 340 and in non-human primates with titers up to 1030.
Extensive surveys on the prevalence of anti-AAV antibodies in humans have been published. Results from these studies indicate that prevalence varies dependent on serotype, and that a significant proportion of individuals develop humoral immunity against various AAV serotypes early in life, starting around 2 years of age. Furthermore, the prevalence of antibodies to different AAV serotypes has been reported to vary according to geographical location.
Study Objective
We performed a NABs seroprevalence study in South African hemophilia B patient population (n=44) using a panel of AAV serotypes suitable for liver targeted therapy, to determine the AAV serotypes likely to be of greatest clinical applicability for the South African hemophilia B population.
Methods
Forty-four hemophilia B patient serum samples were obtained from Hemophilia Comprehensive Care Center in Johannesburg (South Africa). All the patient serum samples were analyzed for the presence of NABs against AAV serotypes 1, 2, 5, 6 and 8 with the use of highly sensitive luciferase-based bioassays. The assays entail incubation of the test serum samples dilution series with an AAV1, 2, 5, 6 or 8-based reporter vector that carries the luciferase gene. This incubation allows neutralizing antibodies in the test serum to bind to the reporter vector particles. These mixtures are subsequently transferred onto Hek293T cells, where reporter vector particles can transduce cells and mediate expression of luciferase. Anti-AAV1, 2, 5, 6 or 8 NABs titers were determined by calculation of the percentage of neutralization for each sample dilution and fitting the neutralization curve with a four-parameter method. Anti-AAV1, 2, 5, 6 or 8 NABs titer (IC50) is the dilution at which antibodies inhibit Hek293T cell transduction with AAV1, 2, 5, 6 or 8-LUC by 50%. The lowest patient serum dilution used in every assay was 8 and samples were considered positive when calculated anti-AAV NAB titer was ≥8. All analytical runs included proper negative and positive controls.
Results and Discussion
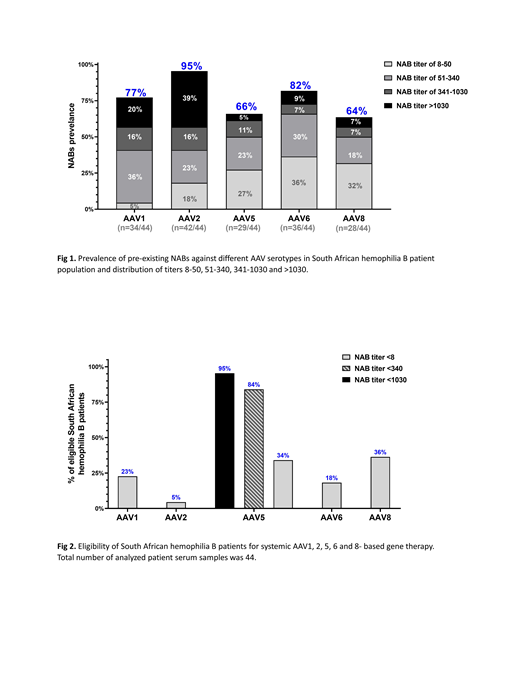
The presence of NABs against the AAV serotypes 1, 2, 5, 6 and 8 was determined in the serum of the hemophilia B patients (Fig. 1). The highest prevalence of NABs was found to be against the AAV2 serotype, 95% (n=42/44) followed by the AAV6 serotype, 82% (n=36/44), and the AAV1 serotype 77% (n=34/44). The prevalence of NABs against AAV5 and AAV8 was lower with 66% (n=29/44) for AAV5 and 64% (n=28/44) for AAV8.
The serum samples positive for anti-AAV2 NABs had a high occurrence of titers above 1030 (39%) in comparison to anti-AAV1 NABs (20%), anti-AAV5 NABs (5%) or anti-AAV8 NABs (7%).The occurrence of samples with low titers (ranging from titer of 8 to titer of 50) was the highest for anti-AAV8 NABs (32%) and for anti-AAV5 NABs (27%), followed by anti-AAV2 (18%) and anti-AAV1 (5%) (Fig.1).
Currently, an anti-AAV NABs titer of 5 is used as an exclusion criteria in most of the systemic AAV-based gene therapies. When applying a similar cut-off of 8, 23% of the analyzed patients could be treated with AAV1, 5% with AAV2, 34% with AAV5, 18% with AAV6 and 36% with AAV8-based therapeutics (Fig.2). However, we have previously reported that AAV5-neutralizing antibodies do not impair the efficacy of in vivo transduction of AAV5-based vector up to a measured titer of 340 in humans and 1030 in non-human primates. Therefore, applying the cut-off of 340 or 1030, either 84% or 95% of the South African Hemophilia B patients could benefit from treatment with AAV5-based gene therapy (Fig.2).
Majowicz:uniQure N.V.: Employment. van Waes:uniQure N.V.: Employment. Timmer:uniQure N.V.: Employment. van Deventer:uniQure Biopharma B.V.: Employment. Mahlangu:Takeda: Consultancy, Honoraria, Speakers Bureau; LFB: Consultancy; NovoNordisk: Consultancy, Research Funding, Speakers Bureau; Roche: Consultancy, Research Funding, Speakers Bureau; Baxalta: Consultancy, Research Funding, Speakers Bureau; Freeline Therapeutics: Research Funding; Pfizer: Consultancy, Research Funding, Speakers Bureau; Spark: Consultancy, Speakers Bureau; Chugai: Consultancy; Biomarin: Research Funding; CSL Behring: Consultancy, Research Funding, Speakers Bureau; Novartis: Research Funding; Sanofi Genzyme: Research Funding, Speakers Bureau; Shire: Consultancy, Research Funding, Speakers Bureau; Sobi: Research Funding, Speakers Bureau; uniQure: Research Funding; World Federation of Haemophilia: Speakers Bureau. Ferreira:uniQure N.V.: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal