


Background and Objectives: Bacterial sepsis is a common complication in pediatric patients with acute myeloid leukemia (AML) undergoing intensive myelosuppressive chemotherapy. Up to 60% of children experience at least one documented infectious complication during therapy, with bacterial causes being most common; infection related mortality may reach 11% (Sung et al, Pediatric Blood & Cancer, 2008). Randomized controlled trials in children undergoing intensive chemotherapy have demonstrated a reduction in bacteremia risk with prophylactic levofloxacin use. This study evaluates epidemiologic data regarding factors associated with levofloxacin use, the impact of levofloxacin on infectious outcomes and the cost-effectiveness of this strategy.
Methods: We queried the Pediatric Health Information System (PHIS) database, which collects billing and coding data from 52 pediatric hospitals, for inpatient encounters of children with AML admitted for chemotherapy with a length of stay ≥14 days from 2013-2018. We collected demographics, information on infectious outcomes and utilization of hospital resources. Variables were compared between children who received levofloxacin prophylaxis during their hospitalization and those who did not using chi-square or Fisher's exact test for categorical variables and t-test of means for continuous variables.
We next developed a decision model comparing levofloxacin prophylaxis through count nadir until recovery to no prophylaxis during a single chemotherapy cycle for AML using published data from randomized controlled trials. We assumed bacteremia was present only in the setting of fevers. We used published literature to estimate the probability of ICU admission or death with or without bacteremia. It was assumed that antibacterial prophylaxis only altered the probabilities of febrile neutropenia and bacteremia. Strategies were compared to analyze incremental costs per bacteremia episode avoided, ICU admission avoided and death avoided. Medication costs were obtained from the Federal Supply Schedule. Costs related to infectious complications and ICU admissions were obtained for patients with AML from PHIS during the 2018 calendar year. Multiple sensitivity analyses tested the robustness of results.
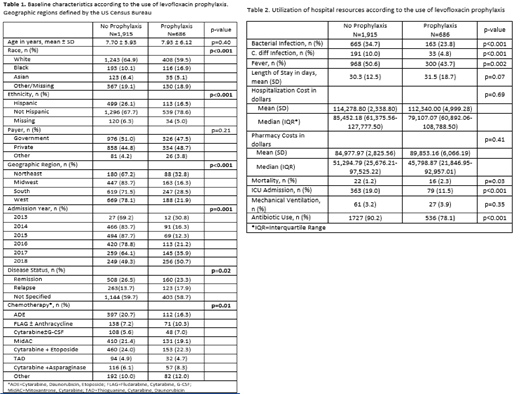
Results: Overall, 26.3% of children received levofloxacin prophylaxis. The decision to use prophylaxis varied significantly by geographic division, AML disease status, year of admission and chemotherapy regimen (Table 1). Patients who received prophylaxis had decreased risk of bacterial infection, C. diff infection, ICU admission and overall antibiotic exposure, not including levofloxacin, during that encounter (Table 2). There was no significant difference between groups regarding length of stay or hospitalization costs.
In PHIS, each bacteremia episode added an average of $119,478 to hospitalization costs. Using baseline probabilities from our literature review, levofloxacin prophylaxis cost $7,252 per bacteremia episode avoided compared with no prophylaxis. This resulted in cost savings of over $100,000 with prophylaxis as the favored strategy. When probabilities for each parameter in the model were altered by 1-way sensitivity analyses, results were sensitive to variation in bacteremia risk with prophylaxis, febrile neutropenia risk, levofloxacin cost and the cost of levofloxacin-related adverse events. However, none of the variations in parameter values generated a result which exceeded a cost-effectiveness threshold of $50,000 per bacteremia episode avoided. In a probabilistic sensitivity analysis, when all parameters were varied simultaneously over the distribution of their potential probabilities, the probability that levofloxacin use was cost-effective at a willingness-to-pay threshold of $50,000 was 95.1%. When considering other outcomes, levofloxacin prophylaxis cost $73,088 per ICU admission avoided compared to actual added costs of $94,181, or $198,525 per death avoided.
Conclusions: Based on available evidence, antibacterial prophylaxis with levofloxacin is effective in reducing bacterial sepsis in pediatric AML patients undergoing intensive chemotherapy. Levofloxacin prophylaxis may also be cost saving when the costs of infectious complications and other adverse health outcomes are considered.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal