

Background .There has been a decrease in the use of unrelated cord blood transplants (UCBT) in the past years: this is probably due to slow hematologic and immune recovery, resulting in a relatively high non relapse mortality (NRM). The addition of anti-thymocyte globulin (ATG) in the conditioning prevents graft versus host disease (GvHD) but makes immune recovery very slow. In addition there is a growing competition of unmanipulated haploidentical transplants.
Aim of the study. We have opened a pilot study to test whether high dose post-transplant cyclophosphamide (PT-CY) would prevent GvHD but still allow for robust immune and hematologic recovery .
Methods. We have grafted 10 patients with an unrelated CB unit and PT-CY. The conditioning regimen was thiotepa (10 mg/kg), busulfan 9.6 mg/kg and fludarabine 150 mg/m^2 (TBF). GvHD prophylaxis was cyclosporin (CSA) starting day 0 (3 mg/kg/day(i.v.), mycophenolate (MMF) 30 mg/kg starting day +1 (p.o) , and PT-CY 30 mg/kg days +3 and +5. The median patients' age was 58 (43-66), and the median weight was 75 kg (54-85) the diagnosis was AML in 8 patients, Ph'+ALL in one and RAEB in one patient; 6 patients were in remission and 4 had active disease.
CB units. The HLA matching of the CB unit was 5/8 antigens/alleles (A,B,C,DRB1) in six patients, 4/8 in two and 2/8 in one. The median nucleated cell dose was 3.1x10^7/kg (range 1.8- 4.5). The ABO was mismatched in all 10 patients.
Hematologic recovery: median time to neutrophils 0.5x10^9/l was day 23 days (range 17-27) and the median time to a platelet count of 20x10^9/L was 38 days (range 34-40). The median counts on day +50 were as follows: Hb 9,1 gr/dL (range 8.7-11.1), Neutrophils 2,3 x10e9/L (range 1-5), PLTs 56 x10e9/L (10-90). One patient failed to engraft and received a second transplant from an unrelated donor, which was successful. No patient developed pure red cell aplasia despite 9/10 being ABO major mismatched.
CD4 recovery : the median CD4 count on day +50 was 74 /cmm (range 67-116) and on day +100 it was 111/cmm(range 100-136). CMV pre-emptive therapy occurred in 3/6 evaluable patients
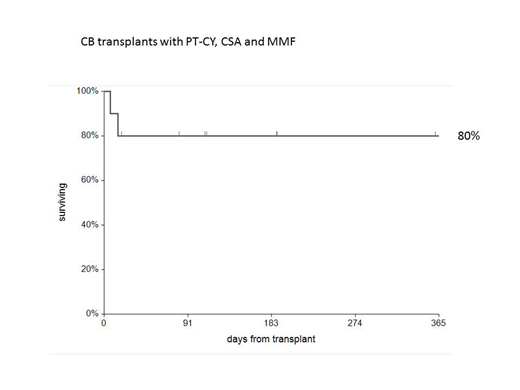
Outcome: two patients with advanced disease, died early of infections, within day +20. GvHD was seen in 1 patient as a transient rash. No patient was treated for GvHD. No patient developed chronic GvHD. No patient relapsed. Eight patients survive in remission, with a median follow up of 6 months, and a projected one year actuarial survival of 80%. Readmissions were extremely rare.
Conclusions. These first 10 patients suggest that UCBT followed by PT-CY, CSA, MMF, as GvHD prophylaxis is feasible and leads to encouraging hematologic and immunologic recovery. We were particularly impressed with the lack of GvHD, the absence of relapses and the good quality of life.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal