

Introduction: Autologous stem cell transplant (ASCT) is a very effective treatment in AL amyloidosis. However, its role is challenged by novel, powerful, non-transplant therapy, also due to the potentially high treatment-related mortality (TRM) that requires an extremely careful patient selection. Bortezomib-based induction and consolidation preceding and following ASCT have been proposed to improve patient outcomes. Here we report the outcome of 139 patients treated with bortezomib-based induction followed by ASCT in case of unsatisfactory response.
Methods: Starting in 2009 we offered upfront therapy with cyclophosphamide (300 mg/m2), bortezomib (1.3 mg/m2) and dexamethasone (40 mg) weekly (CyBorD) to all patients with AL amyloidosis who met the eligibility criteria for transplantation at our institution. Eligibility criteria for ASCT were: age < 65 years, NT-proBNP <5000 ng/L, eGFR >50 mL/min per 1.73 m2, NYHA class >3, PS-ECOG, ≤2, left ventricular EF >45%, DLCO >50% (Palladini and Merlini, Blood 2016). Patients who did not achieve a satisfactory response after CyBorD proceeded to ASCT (with melphalan 200 mg/m2), if still eligible. A satisfactory response was defined as complete response (CR), very good partial response (VGPR) with organ response (OR), or partial response (PR) with OR. Patients with overt multiple myeloma were excluded. We assessed response rates (by intent-to-treat), overall survival (OS) and time to next line of treatment or death (TNTD).
Results: Between 2009 and 2018, 139 consecutive newly diagnosed patients were eligible for ASCT and received CyBorD as first line treatment. They represented 15% of all patients diagnosed at our center during the study period. Patients' characteristics are reported in Table 1. Treatment with CyBorD continued for 2 cycles in 44 patients (32%), 4 cycles in 64 (46%), 6 cycles in 20 (14%) and 8 cycles in 11 (8%) patients. Only one patient (stage IIIa) died within 100 days from CyBorD initiation due to sudden death.
After CyBorD treatment, 26 (20%) patients achieved CR, 45 (32%) VGPR, and 24 (17%) PR (overall hematologic response rate 69%). Sixty-three patients (45%) achieved a satisfactory response after CyBorD and did not proceed to ASCT. Twenty-one patients (15%) who did not reach a satisfactory response after CyBorD did not proceed to ASCT because of organ progression that made them no longer eligible (16 subjects, 12%) or patient refusal (5 cases, 4%). The remaining 55 subjects (40%) received ASCT. No patients died within 100 days from ASCT. Hematologic response after ASCT was obtained in 80% of patients, with CR in 21 subjects (38%), VGPR in 15 (27%) and PR in 8 (15%). In the overall cohort, the hematologic response rate after CyBorD or CyBorD followed by ASCT was 77%, with 47 subjects (34%) attaining CR, 40 (29%) VGPR, and 19 (14%) PR.
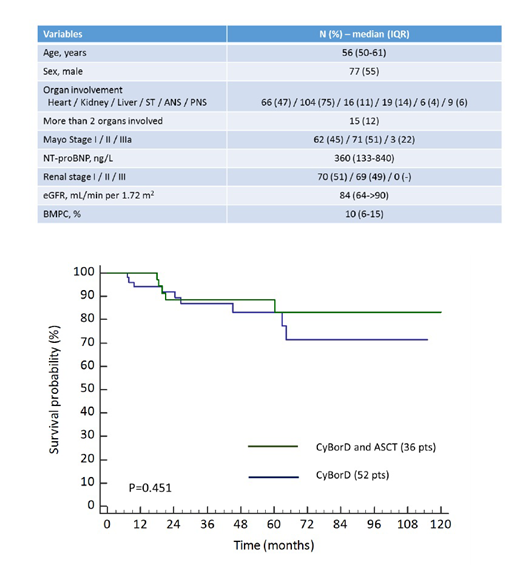
After a median follow-up of living patients of 48 months, 27 subjects died. In the whole study cohort, overall median survival (OS) was not reached and projected OS was 78% at 4 years and 69% at 10 years. In patients who proceeded to ASCT, median OS was not reached, and projected survival was 90% at 4 years and 77% at 10 years. In patients who achieved a satisfactory response after CyBorD and did not proceed to ASCT, median OS was not reached as well, and projected survival was 84% at 4 years and 72% at 10 years (P=0.438 compared to ASCT). In patients who did not proceed to ASCT despite having failed to achieve a satisfactory response after CyBorD, median survival was 47 months (P<0.001 compared to the 2 other groups). We then compared OS in patients who achieved VGPR or CR after CyBorD alone or after CyBorD followed by ASCT and found no significant difference (Figure 1). Finally, we evaluated TNTD in patients who attained CR and found no significant difference between subjects treated with CyBorD alone and those who received ASCT after CyBorD (relapsed or dead at 4 years 36% vs. 20%, P=0.737). This is in agreement with the median time to relapse from CR of 4.3 years reported by the Boston University group (Browning, et al. Blood 2017).
Conclusion: This sequential treatment approach granted a high rate of profound hematologic responses and prolonged survival with minimal TRM (<1%) that occurred during the induction phase. In patients who attained profound hematologic response (CR or VGPR), OS and durability of response were similar in subjects who responded to initial CyBorD and in those who proceeded to ASCT.
Milani:Janssen: Honoraria; Pfizef: Honoraria. Palladini:Sebia: Honoraria; Celgene: Other: Travel grant; Janssen-Cilag: Other: Travel grant; Janssen-Cilag: Honoraria.
Bortezomib in AL amyloidosis

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal