

Background: Carfilzomib and Bendamustine are currently FDA approved for therapy of relapsed refractory multiple myeloma (MM). Bendamustine, in addition to interference with DNA replication, it can induce inhibition of mitotic checkpoints, inefficient DNA repair, and initiation of a p53-dependent DNA-damaging stress response leading to apoptosis of tumor cells (1). It has previously shown significant activity in relapsed myeloma (2). Carfilzomib is a second generation, irreversible proteasome inhibitor has demonstrated promising activity in first line therapy (3,4). we hypothesized that combining them will yield an effective induction regimen in the newly diagnosed MM.
Study design: Inclusion criteria included newly diagnosed MM with measurable disease, age ≥18, ECOG PS 0-2, adequate renal (creatinine clearance >30 mL/min), cardiac and hepatic function. Carfilzomib was given IV on days 1, 2, 8, 9, 15, 16. All patients received 20 mg/m2 on days 1 and 2 of cycle 1, after which their dose was escalated to one of the following levels: 27, 36, 45, or 56 mg/m2. Bendamustine IVPB on days 1, 2, at 70 (dose levels 1 and 2) or 90 mg/m2 (dose levels 3-5). Dexamethasone 20 mg PO or IV D 1, 2, 8, 9, 15, 16, 22, 23. Each cycle of therapy was 28 days, and a total of 8 cycles was given. Stem cell harvest was done after 4 cycles and eligible patients proceeded to ASCT after 8 cycles. Maintenance was recommended - either carfilzomib (36mg/m2 D 1,2, 15, 16 of a 28-day cycle for 2 years, or investigator's choice. Primary objective was to determine the recommended phase 2 dose (RP2D) and additional objectives assessed efficacy and safety.
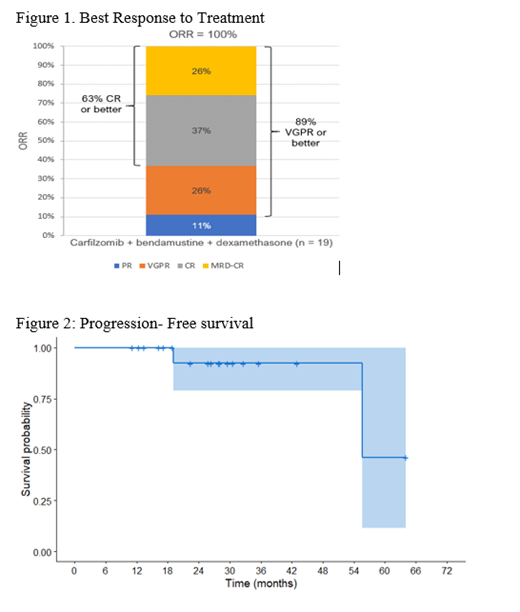
Results: Between February 2014 and May 2018, 20 patients with newly diagnosed MM pts were accrued onto study (5 pts in phase I and 15 in phase II). Median age was 65 (range 48-74), and 14 (70%) patients were male. 7 (35%) were of Hispanic ethnicity. 3 patients (15%) were R-ISS stage 3, and 1 (5%) had high-risk cytogenetics. We did not observe any DLTs with our study treatment and established the RP2D as: carfilzomib 56 mg/m2, bendamustine 90 mg/m2 and dexamethasone 20 mg on the dosing schedule given above. The most common and severe toxicities were hematologic. Grade 3/4 hematologic toxicities were lymphocytopenia in 90% of patients, neutropenia 40%, anemia 20% and thrombocytopenia 20%. Notable non-hematologic toxicities were grade 3/4 infection in 20% of patients (typically upper respiratory and pneumonia), grade 1/2 acute kidney injury in 45% of patients, and grade 1/2 diarrhea in 40% of patients. No treatment emergent hypertension or heart failure were noted. 1 patient died while on study, from septic shock due to pneumonia 7 weeks after completion of induction. The regimen was highly effective, with an ORR of 100%. Best responses were: 2 (11%) PR, 5 VGPR (26%), and 12 CR (63%) (Figure 2). Among the CRs, 4 were MRD-positive, 5 were MRD-negative, and 3 did not have MRD testing. With a median follow-up of 28 months (range 11-71), 2 patients have progressed - 1 with del(17p) at 19 months after diagnosis, and the other with standard cytogenetic risk disease at 56 months. 2 patients have died - the patient with del(17p) from refractory myeloma at 37 months after diagnosis, and the other from septic shock as discussed above. Median PFS was 56 months, and median OS has not been reached.
Conclusion: Carfilzomib, Bendamustine and Dexamethasone is safe and highly effective for newly diagnosed transplant eligible MM and should be further explored in a larger prospective trial for this patient population.
References:
1. Leoni LM, Hartley JA. Mechanism of action: the unique pattern of bendamustine-induced cytotoxicity. Seminars in hematology 2011;48 Suppl 1:S12-23.
2. Lentzsch S, O'Sullivan A, Kennedy RC, et al. Combination of bendamustine, lenalidomide, and dexamethasone (BLD) in patients with relapsed or refractory multiple myeloma is feasible and highly effective: results of phase 1/2 open-label, dose escalation study. Blood 2012;119:4608-13.
3. Dimopoulos MA, Goldschmidt H, Niesvizky R, et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): an interim overall survival analysis of an open-label, randomised, phase 3 trial. The Lancet Oncology 2017;18:1327-37.
4. Jakubowiak AJ, Dytfeld D, Griffith KA, et al. A phase 1/2 study of carfilzomib in combination with lenalidomide and low-dose dexamethasone as a frontline treatment for multiple myeloma. Blood 2012;120:1801-9.
Bhutani:Sanofi: Membership on an entity's Board of Directors or advisory committees. Assal:Incyte corporation: Consultancy, Research Funding; boston biomedical: Consultancy. Lentzsch:Janssen: Consultancy; Takeda: Consultancy; BMS: Consultancy; Proclara: Consultancy; Abbvie: Consultancy; Clinical Care Options: Speakers Bureau; Sanofi: Consultancy, Research Funding; Multiple Myeloma Research Foundation: Honoraria; International Myeloma Foundation: Honoraria; Karyopharm: Research Funding; Columbia University: Patents & Royalties: 11-1F4mAb as anti-amyloid strategy; Caelum Biosciences: Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Bayer: Consultancy.
Carfilzomib, Bendamustine and Dexamethasone for newly diagnosed multiple myeloma.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal