

BACKGROUND: Phase 3 trials and a meta-analysis have demonstrated that Lenalidomide (Len) administration as maintenance improves the PFS and OS after ASCT performed as part of 1st line therapy. In addition, retrospective and registry studies have suggested efficacy when post-ASCT maintenance is administered after salvage ASCT in relapsed patients. Len maintenance has become the standard approach in many centres, including in Canada where it is routinely funded after 1st line ASCT and Len-base regimens are often used as maintenance after salvage ASCT in pts who have not progressed on this agent previously. The optimal management of patients (pts) progressing on this highly effective agent is less clear, however. We utilized the MCRN Database to investigate which regimens were utilized after pts progressed on Len-based therapy (post-Len Rx) and the outcomes observed with such regimens in the real-world Canadian setting. We included pts receiving Len-based regimens as maintenance following ASCT performed as part of 1st, 2nd or 3rd line therapy in this analysis, as ASCT pts are relatively young and generally tolerate combination regimens for relapsed myeloma well.
METHODS: The MCRN Database is an ongoing national Canadian web-based repository of detailed information on over 6000 myeloma patients from 13 academic centres dating back to 2007. In this analysis, we evaluated the characteristics of pts progressing on post-ASCT Len-based maintenance following a transplant performed as part of the first 3 regimens administered. Pts were treated between 01/2007 until 04/2019; 305 pts had undergone 1 ASCT, 59 pts had 2 ASCTs. The next -line therapy administered at this time (post-Len Rx) was classified based on the novel agent utilized. Overall response rates (ORR), PFS from start of post-len Rx to next progression and OS (calculated from post-Len Rx to death) was calculated for these pts. Categorical comparisons were performed using the chi-square test and continuous ones using ANOVA. Survival rates were calculated using the Kaplan-Meier product-limit method; comparisons among regimens were made using the log-rank statistic.
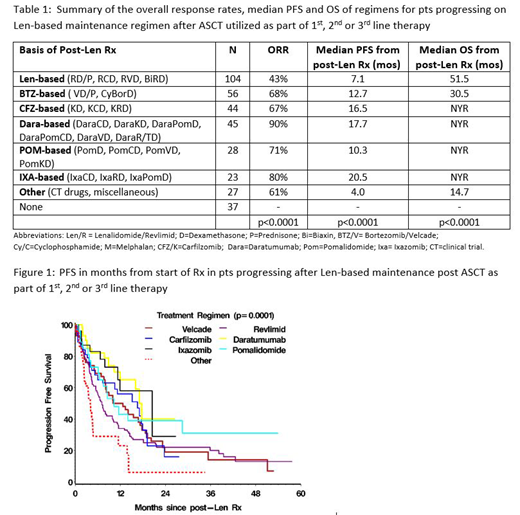
RESULTS: We identified 364 pts who had progressed on Len-based regimens given for maintenance, after ASCT, including 306 after 1st line ASCT, 51 after 2nd line ASCT and 7 after 3rd line ASCT. Len-based maintenance included Len alone in 318, Len + dex in 24 and other Len-combinations in 22. Median age was 59 yrs, 58% were male, 43.6% of 243 evaluable pts had high-risk FISH cytogenetics (del 17p, t[4;14], t[14;16]). Median creatinine was 85 µmol/L (32-832), LDH 187 U/L (55-906) and B2M 295 nmol/L (1.8-3805). Post-Len Rx was based on bortezomib (BTZ) in 56 (15%), carfilzomib (CFZ) in 44 (12%), daratumumab (Dara) in 45 (12%), pomalidomide (POM) in 28 (8%), ixazomib (IXA) in 23 (6%), and other regimens in 27 (7%). Thirty-seven (10%) did not receive any post-Len therapy while 104 (28%) received further Len-based therapy with the addition of Dex alone in 73, or with an additional agent (BTZ, cyclophosphamide [Cy] and/or clarithromycin) in 31 (Table 1). The only significant difference in pt characteristics was a higher LDH value in the IXA and POM groups (p=0.0015).
The median PFS of 327 patients who received treatment for progression on Len-based maintenance was 11 months (mos) (95% CI 8.1-13.9); OS was 39 mos (95% CI 31-60) from post-Len Rx. For the 92 (42%) pts with high-risk FISH, the median PFS was 7.9 mos (95%CI 5.3 -11.5) and OS 33 mos (95%CI > 23.7) compared with 11.9 mos (95%CI 8.1 -14.2) and 39.7 mos (95% CI>23.9) respectively, for standard-risk pts. The ORR, median PFS and OS of each regimen from the time of post-Len Rx are summarized in Table 1, Fig 1.
CONCLUSIONS: 1) the median PFS with post-Len Rx in pts progressing on Len-based maintenance after ASCT as part of 1st, 2nd or 3rd line treatment was almost 1 year for all treated pts, with longer benefit observed in pts treated with the newer proteasome inhibitors or Dara-based regimens; 2) since there was potentially confounding overlap among the agents in used in each treatment group studied-- and the 1st, 2nd and 3rd line transplant settings involved different time points in the disease course--further subset analyses of specific regimens/settings are ongoing; 3) nevertheless, the overall real-world results observed with newer agents approximate the outcomes reported in clinical trials in pts progressing on Len-based regimens after 1-3 prior lines of therapy.
Reece:Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Research Funding; Takeda: Consultancy, Honoraria, Research Funding; BMS: Research Funding; Karyopharm: Membership on an entity's Board of Directors or advisory committees, Research Funding; Otsuka: Research Funding; Amgen: Consultancy, Honoraria, Research Funding. McCurdy:Celgene: Honoraria; Janssen: Honoraria. Song:Celgene: Honoraria, Research Funding; Janssen: Honoraria; Amgen: Honoraria; Takeda: Honoraria. Leblanc:Janssen: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees. Sebag:Amgen: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees. White:Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria. Stakiw:Janssen: Honoraria, Research Funding, Speakers Bureau; BMS: Honoraria; Amgen: Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Celgene: Honoraria, Speakers Bureau; Roche: Research Funding; Lundbeck: Honoraria; Sanofi: Honoraria. Louzada:Janssen: Consultancy, Honoraria; Bayer: Honoraria; Celgene: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Amgen: Consultancy, Honoraria. Kotb:Merck: Honoraria, Research Funding; Janssen: Honoraria; Amgen: Honoraria; Karyopharm: Equity Ownership; Celgene: Honoraria; Takeda: Honoraria. Venner:Sanofi: Honoraria; Janssen: Honoraria; Amgen: Honoraria, Research Funding; Takeda: Honoraria; Celgene: Honoraria; J&J: Research Funding.
This abstract describes several combinations not specifically approved by the FDA but utilized in the real-world setting. However, all of the individual drugs in these combinations have been approved as single agents or in other combinations.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal