

Background
Multiple myeloma (MM), a malignant neoplasm of plasma cells in the bone marrow, accounts for up to 1.8% of all cancers in the U.S., most frequently affecting people 65-74 years old. A variety of therapies are available to manage MM, including stem cell transplantation (SCT), immunomodulatory drugs (IMiD), proteasome inhibitors (PI), monoclonal antibodies (mAB), and alkylating agents (alk). Given the heterogeneity of MM and the rapidly evolving therapeutic landscape, MM contemporaneous real-world treatment patterns are not well described. We examined the patient characteristics and first-line (LT1) treatment patterns in NDMM patients.
Methods
MM patients (≥18 years), diagnosed in April 30, 2015 - April 29, 2017 (early cohort) or in April 30, 2017 - April 30, 2019 (recent cohort), were followed retrospectively from MM diagnosis to last patient activity in the Flatiron Health database - a geographically-diverse, longitudinal electronic health record spanning over 280 community and academic cancer clinics in the U.S. LT1 regimens were described as: 1) containing an IMiD (thalidomide, lenalidomide [R], or pomalidomide), PI (bortezomib [V], carfilzomib, or ixazomib), alk (melphalan, cyclophosphamide [C], bendamustine), mAB (daratumumab, elotuzumab), or combinations of these; and 2) doublet/monotherapy (doublets-) vs. triplet or greater agent (triplets+) combinations. Treatment patterns were examined by SCT status and by cytogenetic risk (high: del17p, t(4;14) and/or t(14;16); standard: ≥1 cytogenetic tests without high cytogenetic risk) and age groups (<65, 65-74, ≥75). Duration of therapy (DOT) and time to next therapy (TTNT) were estimated using Kaplan-Meier methods in the early cohort with longer follow-up.
Results
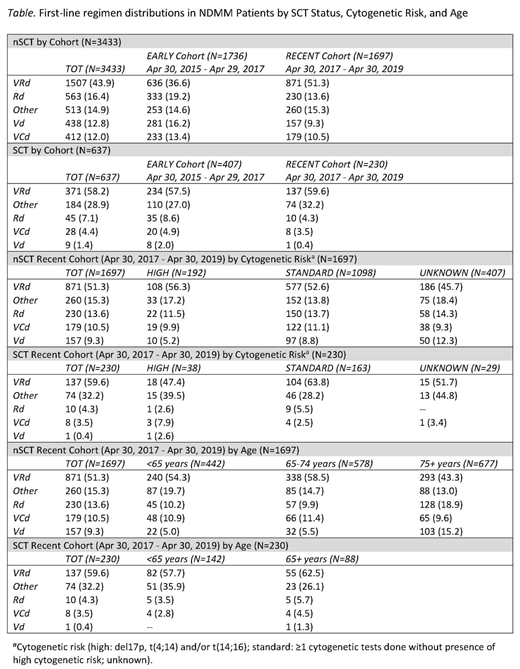
Of 4,070 NDMM patients, 3,433 were non-SCT (nSCT: early cohort: n=1,736; recent cohort: n=1,697) and 637 had SCT (early cohort: n=407; recent cohort: n=230). In nSCT patients, mean age at diagnosis was 70 years (SD: 10); 46% were female; 36% had stage III (699/1916, among non-missing), and 15% (392/2574, among non-missing) had high risk MM (25% had unknown cytogenetics). SCT patients were younger at diagnosis (mean [SD]: 61 years [9]); 44% were female; 25% (117/470, in non-missing) had stage III, and 19% (102/547, in non-missing) had high risk MM (14% had unknown cytogenetics). Overall, proportions with known cytogenetic risk were similar within SCT status cohorts over time but were lower in the SCT group (nSCT early vs. recent cohort: 26% vs. 24% had unknown cytogenetics; and in SCT: 15% vs. 13%, respectively). In nSCT and SCT patients, respectively, most common regimens were VRd (d: dexamethasone; 44% and 58%), Rd (16% and 7%), Vd (13% and 1%), and VCd (12% and 4%). In nSCT patients, the use of VRd increased over time (37% [early cohort] to 51% [recent cohort]), while frontline therapy with Rd/Vd doublets (19% to 14%/16% to 9%) and with VCd (13% to 11%) decreased. In the nSCT recent cohort, VRd (51%) frontline therapy dominated, with a slightly higher proportion of patients in the high-risk group vs. standard and unknown risk receiving VRd (56% vs. 53% and 46%); use of doublet therapy with Rd/Vd was lower in the high risk (12%/5%) vs. standard risk group (14%/9%). Irrespective of age, VRd was the most common frontline regimen in the nSCT recent cohort, albeit its use was lower among patients 75+ years of age (43%) vs. younger patients (54% [<65 years] and 59% [65-74 years]); 75+ year old patients had a higher use of Rd/Vd doublets (19%/15%) vs. <65 (10%/5%) or 65-74 (10%/6%) years of age. Triplets+ were more commonly used than doublets- across all cohorts: 59% vs. 41% (nSCT early cohort); 74% vs. 26% (nSCT recent cohort); and 89% vs. 11% (SCT early cohort); 95% vs. 5% (SCT recent cohort). mAB use in the recent cohort was low: 1.4% nSCT and 2.2% SCT patients. In the nSCT early cohort, the median (95% CI) LT1 DOT was 10 months (9-11) and for TTNT was 14 months (13-16).
Conclusions
PI/IMiD treatment combinations were most commonly observed in both nSCT and SCT patients, with an increase in use from early (40%) to recent (56%) cohort in nSCT patients. Use of triplets, generally, is on the rise from early (60%) to recent cohorts (74%). LT1 TTNT was lower than has been shown in clinical trials. These findings indicate a notable change in treatment patterns over time in nSCT NDMM patients, highlighting the changing landscape of MM management.
Ailawadhi:Celgene: Consultancy; Takeda: Consultancy; Cellectar: Research Funding; Amgen: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Pharmacyclics: Research Funding. Romanus:Takeda: Employment. Cherepanov:Takeda: Employment. Yin:Takeda: Employment. Cheng:Takeda: Employment. Hari:Celgene: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Research Funding; Janssen: Consultancy, Honoraria; Kite: Consultancy, Honoraria; Amgen: Research Funding; Spectrum: Consultancy, Research Funding; Sanofi: Honoraria, Research Funding; Cell Vault: Equity Ownership; AbbVie: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal