

Introduction
Chimeric Antigen Receptor T cells (CAR-T) therapy, e.g. B Cell Maturation Antigen (BCMA)-directed CAR-T has provided an encouraging modality for relapsed and refractory management of multiple myeloma (MM). However, a significant portion of patients still relapse with progressive disease after monospecific anti-BCMA CAR-T treatment. It has been demonstrated that CD19-directed CAR-T was effective in certain MM patients, likely due to CD19 expression on subsets of MM cells, and/or undetectable level of CD19 on MM cells. In addition, it has been reported that CD19 could express on the myeloma progenitor cells. To further improve the efficacy and to reduce relapse, we have designed a bispecific CAR-T targeting both BCMA and CD19. In addition to the conventionally-manufactured BCMA-CD19 CAR-T, the bispecific CAR-T was also successfully manufactured in our newly developed FasT CAR-T platform, which shortened the production time to one day. Here we report the results from pre-clinical studies and early results from the first-in-human clinical study.
Methods
The BCMA-CD19 bispecific CAR was constructed by linking BCMA and CD19 scFv, joined by a CD8 hinge, transmembrane domain, co-stimulatory domain and CD3. CAR-T cells were produced using either the conventional process (GC012) or the FasT CAR-T platform (GC012F). Peripheral blood (PB) mononuclear cells were obtained by leukapheresis either from healthy donors for the pre-clinical study or from patients for the clinical trial. T cells were isolated and used for CAR-T manufacturing. A xenograft mouse model was used to determine the efficacy in vivo.
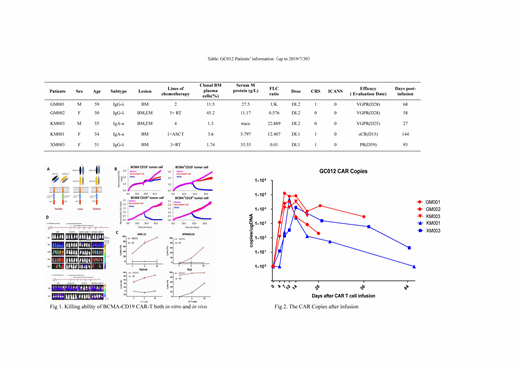
From March 2019 to July 2019, 5 adult relapsed/refractory MM patients (Age 50-59), who had previously received multiple lines of therapies, were enrolled (Table). Among them, 2 had extramedullary diseases. One patient did not receive lymphodepletion, and all other 4 patients received i.v. fludarabine and cyclophosphamide for 3 days. All patients received a single infusion of CAR-T cells, either at dose 1x106/Kg (DL1) (2 patients) or at dose 2x106/Kg (DL2) (3 patients), and the dose escalation is still ongoing. The endpoints of the exploratory trial were to evaluate the safety, feasibility, PK, and clinical efficacy of BCMA-CD19 bispecific CAR-T.
Results
In pre-clinical study, BCMA-CD19 bispecific CAR-T were very effective in killing CD19+ and/or BCMA + target cells including MM cell lines RPMI8226 and MM.1s (Fig 1). Increased IFN production and CD107a up-regulation were also observed. We demonstrated that BCMA-CD19 CAR-T completely eliminated BCMA+ MM cell line RPMI8226, MM.1s, and CD19+ ALL cell line Nalm6 in in vivo xenograft models. Additionally BCMA-CD19 CAR-T cells were shown to be more cytotoxic than single CAR-T both in vitro and in vivo. BCMA-CD19 CAR-T manufactured in the FasT CAR-T platform was more effective in eliminating MM in a xenograft model (Fig. 1).
In the clinical study, the median observation time was 68 days (27-144 days up to 2019/7/30). Five patients were evaluated between 15-59 days post CAR-T infusion. Despite the relatively short disease evaluation time, all 5 patients responded to the treatment: 1 patient achieved sCR, 3 achieved VGPR and 1 achieved PR. Notably, although patient KM001 did not receive any pre-conditioning, however, the patient achieved sCR status on Day 15 and has maintained sCR up to now (129 days). CAR-T PK in the PB was monitored by qPCR and flow cytometry. The CAR-T proliferation peak was reached on Day 10 (D7-D14), and the median peak copy number was 34,039 (12,897-128,775) copies /ug DNA (Fig. 2). Remarkably, despite the encouraging clinical response to the CAR-T treatment, no severe adverse events were encountered during the observation period. Three patients experienced only grade 1 cytokine release syndrome (CRS) and no subject suffered from neurotoxicity of any level (Table).
Conclusion
Pre-clinical data demonstrated BCMA-CD19 CAR-T cells are effective in eliminating MM tumor cells both in vitro and in vivo. The first-in-human clinical trial also showed extraordinary safety profile and efficacy of BCMA-CD19 bispecific CAR-T in treating R/R MM. The long-term benefit and effect on relapse are being further studied. Bispecific CAR-T manufacturing on the FasT CAR-T platform is successful and has been shown to be more potent. A clinical study to evaluate safety and efficacy of FasT BCMA-CD19 CAR-T is ongoing.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal