

Background: Multiple myeloma (MM) is common among the elderly, with 35% of patients (pts) diagnosed being aged ≥75 years (y). With increasing overall life expectancy, the incidence and prevalence of newly diagnosed and previously treated MM patients ≥80 y is expected to increase over time. Because elderly pts are often excluded from clinical trials, data focused on their treatment patterns and clinical outcomes are lacking. The Connect® MM Registry (NCT01081028) is a large, US, multicenter, prospective observational cohort study of pts with newly diagnosed MM (NDMM) designed to examine real-world diagnostic patterns, treatment patterns, clinical outcomes, and health-related quality of life patient-reported outcomes. This analysis reviews treatment patterns and outcomes in elderly pts from the Connect MM Registry.
Methods: Pts enrolled in the Connect MM registry at 250 community, academic, and government sites were included in this analysis. Eligible pts were adults aged ≥18 y with symptomatic MM diagnosed ≤2 months before enrollment, as defined by International Myeloma Working Group criteria; no exclusion criteria were applied. For this analysis, pts were categorized into 4 age groups: <65, 65 to 74, 75 to 84, and ≥85 y. Pts were followed from time of enrollment to the earliest of disease progression (or death), loss to follow-up, or data cutoff date of February 7, 2019. Descriptive statistics were used for baseline characteristics and treatment regimens. Survival outcomes were analyzed using Cox regression. Time to progression (TTP) analysis excluded causes of death not related to MM.
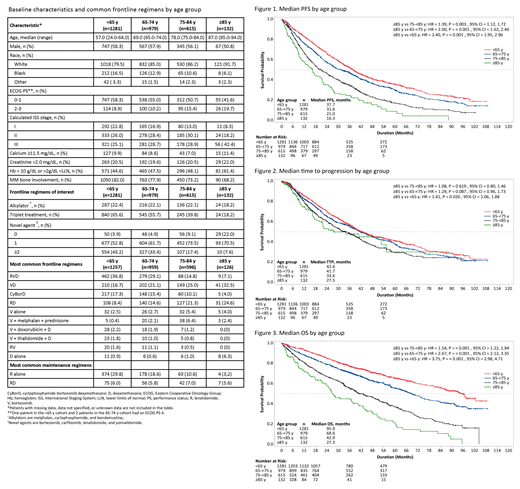
Results: Of 3011 pts enrolled (median age 67 y), 132 (4%) were aged ≥85 y, and 615 (20%) were aged 75-84 y at baseline. More pts aged ≥85 y had poor prognostic factors such as ISS stage III disease and reduced hemoglobin (<10 g/dL or >2 g/dL <LLN) compared with other age groups, although no notable differences between creatinine and calcium levels were observed across age groups (Table). A lower proportion of elderly pts (75-84 and ≥85 y) received triplet regimens as frontline therapy. More elderly pts received a single novel agent, whereas use of 2 novel agents was more common in younger pts (Table). The most common frontline regimens among elderly pts were bortezomib (V) + dexamethasone (D), followed by lenalidomide (R) + D, whereas those among younger pts included RVD, followed by VD and CyBorD (Table). No pt aged ≥85 y, and 4% of pts aged 75-84 y received high-dose chemotherapy and autologous stem cell transplant (vs 61% in the <65 y and 37% in the 65-74 y age group). The most common maintenance therapy was RD in pts ≥85 y (although the use was low) and R alone in other age groups (Table). In the ≥85 y group, 27%, 10%, and 4% of pts entered 2L, 3L, and 4L treatments respectively, vs 43%, 23%, and 13% in the <65 y group.
Progression-free survival was significantly shorter in the ≥85 y age group vs the 75-84 y age group (P=0.003), 65-74 y age group (P<0.001), and <65 y age group (P<0.001; Fig.1). TTP was significantly shorter in the ≥85 y group vs the <65 y group (P=0.020); however, TTP was similar among the 65-74 y, 75-84 y, and ≥85 y cohorts (Fig. 2). Overall survival was significantly shorter in the ≥85 y group vs the 75-84 y, 65-74 y, and <65 y groups (all P<0.001; Fig. 3). The mortality rate was lowest (46%) during first-line treatment (1L) in pts aged ≥85 y (mainly attributed to MM progression) and increased in 2L and 3L (47% and 54%, respectively); a similar trend was observed in the younger age groups. The main cause of death was MM progression (29% in the ≥85 y vs 16% in the <65 y group). Other notable causes of death in the ≥85 y group included cardiac failure (5% vs 2% in <65 y group) and pneumonia (5% vs 1% in <65 y group).
Conclusions: In this analysis, elderly pts received similar types of frontline and maintenance regimens as younger pts, although proportions varied with decreased use of triplet regimens with age. Considering similarities in TTP across the 65-74 y, 75-84 y, and ≥85 y cohorts, these real-world data support active treatment and aggressive supportive care of elderly symptomatic pts, including with novel agents. Additionally, further clinical studies specific to elderly patients with MM should be explored.
Lee:Amgen: Consultancy, Research Funding; GlaxoSmithKline plc: Research Funding; Sanofi: Consultancy; Daiichi Sankyo: Research Funding; Celgene: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding. Ailawadhi:Janssen: Consultancy, Research Funding; Takeda: Consultancy; Pharmacyclics: Research Funding; Amgen: Consultancy, Research Funding; Celgene: Consultancy; Cellectar: Research Funding. Gasparetto:Celgene: Consultancy, Honoraria, Other: Travel, accommodations, or other expenses paid or reimbursed ; Janssen: Consultancy, Honoraria, Other: Travel, accommodations, or other expenses paid or reimbursed ; BMS: Consultancy, Honoraria, Other: Travel, accommodations, or other expenses paid or reimbursed . Jagannath:AbbVie: Consultancy; Merck & Co.: Consultancy; Bristol-Myers Squibb: Consultancy; Karyopharm Therapeutics: Consultancy; Celgene Corporation: Consultancy; Janssen Pharmaceuticals: Consultancy. Rifkin:Celgene: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees. Durie:Amgen, Celgene, Johnson & Johnson, and Takeda: Consultancy. Narang:Celgene: Speakers Bureau. Terebelo:Celgene: Honoraria; Jannsen: Speakers Bureau; Newland Medical Asociates: Employment. Toomey:Celgene: Consultancy. Hardin:Celgene: Membership on an entity's Board of Directors or advisory committees. Wagner:Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; American Cancer Society: Other: Section editor, Cancer journal. Omel:Celgene, Takeda, Janssen: Other: Patient Advisory Committees. Srinivasan:Celgene: Employment, Equity Ownership. Liu:TechData: Consultancy. Dhalla:Celgene: Employment. Agarwal:Celgene Corporation: Employment, Equity Ownership. Abonour:BMS: Consultancy; Celgene: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal