

Background: Triplet combination strategies have widely been accepted as the standard of care for the management of multiple myeloma due to improved outcomes as compared to doublets. The combination of daratumumab, pomalidomide and dexamethasone (DPd) has previously demonstrated deep and durable responses, including high rates of MRD negativity, in a heavily pretreated patient population. Quadruplet regimens offer an opportunity to further improve upon these results. We report preliminary findings from an ongoing phase 2 multicenter trial of the addition of ixazomib to the combination of DPd in patients with relapsed/refractory multiple myeloma. The primary objective is to determine overall response rate and the safety and tolerability of this novel regimen. Key secondary endpoints include PFS, OS and MRD negativity rates.
Methods: Eligible patients may have received ≥1 and ≤3 prior lines of therapy, have had no prior exposure to daratumumab or ixazomib, and may have not progressed on prior pomalidomide. Patients receive daratumumab 16mg/kg IV weekly x 8 doses, biweekly x 8 doses, then monthly, pomalidomide 4mg PO days 1-21/28, ixazomib 4mg PO days 1,8,15 every 28 days, and dexamethasone 40mg PO weekly. Patients continue on therapy until disease progression, intolerability or preference. Dose-limiting toxicities (DLT) were defined as grade 3-4 hematologic adverse events (AE) or any AE that required a dose modification of pomalidomide or ixazomib at the lowest dose levels on a dose de-escalation plan. An interim safety review was performed after the first 6 patients were enrolled and completed the DLT observation period, which is the first cycle (28 days) since the start of a new dose level of pomalidomide and/or ixazomib.
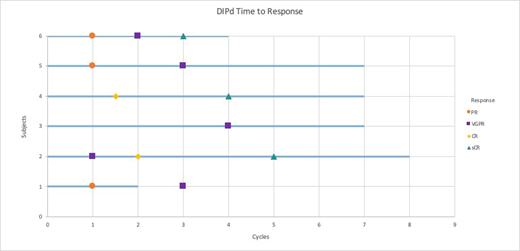
Results: At the time of this analysis, six patients have been enrolled and treated, and completed the DLT observation period. Patients had a median age of 62 (range 52-65) and median number of 2 prior lines of therapy (range 1-2). All patients were refractory to lenalidomide and pomalidomide-naïve. Common adverse events (AEs) included neutropenia, thrombocytopenia, GI upset, and upper respiratory infection. Grade 3-4 AEs were predominantly hematologic including neutropenia and thrombocytopenia, but also included grade 3 hypertension in 1 patient, and grade 3 hypophosphatemia, grade 4 hypokalemia, and grade 3 small bowel infection in 1 patient. No IRR > grade 2 occurred with daratumumab administration. No DLTs occurred in the first six patients in the safety run-in. The overall response rate of the cohort is 100% with 3 patients achieving a stringent complete response (CR), and 3 patients achieving a very good partial response (VGPR) after a median of 7 cycles of treatment. One patient discontinued therapy due to influenza A, the other five remain on therapy. Minimal residual disease assessments are being performed by EuroFlow for patients in VGPR or better due to concern for daratumumab interference. Pharmacodynamic changes in patients' tumor microenvironments were established by custom panel mass cytometry to include T-cell memory and activated subpopulations, B-cell content, NK-cell subpopulations as well as MDSCs, Tregs and T-exhaustive markers, monocytes and dendritic cells.
Conclusion: The quadruplet regimen DIPd in patients with relapsed/refractory myeloma is a well-tolerated combination and has shown early safety in an initial safety run-in analysis. Enrollment continues in an expansion cohort to assess efficacy at multiple sites with the University of California Hematologic Malignancies Consortium.
Costello:Takeda: Honoraria, Research Funding; Janssen: Research Funding; Celgene: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal