

Background: Ibrutinib is the only once-daily Bruton's tyrosine kinase inhibitor with significant progression-free survival (PFS) benefit demonstrated in 5 randomized phase 3 studies in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) compared with standard-of-care chemotherapy and/or immunotherapy (RESONATE, RESONATE-2, iLLUMINATE, Alliance 041202, and ECOG 1912), and significant overall survival (OS) benefit in 3 of these studies. To understand how treatment with single-agent ibrutinib in earlier lines impacts patient outcomes, we evaluated long-term follow-up data from RESONATE and RESONATE-2 to compare efficacy and safety by number of prior lines of therapy.
Methods: This integrated analysis included patients treated with single-agent ibrutinib in the first-line (RESONATE-2, NCT01722487) and relapsed/refractory (R/R; RESONATE, NCT01578707) settings. R/R patients were grouped by number of prior lines of therapy (1-2 vs ≥3). Patients with del(17p) were excluded from this analysis given their exclusion from RESONATE-2. Patients with high-risk prognostic features were defined as having TP53 mutation, del(11q), and/or unmutated IGHV. Outcomes included investigator-assessed PFS and objective response rate (ORR), OS, and safety.
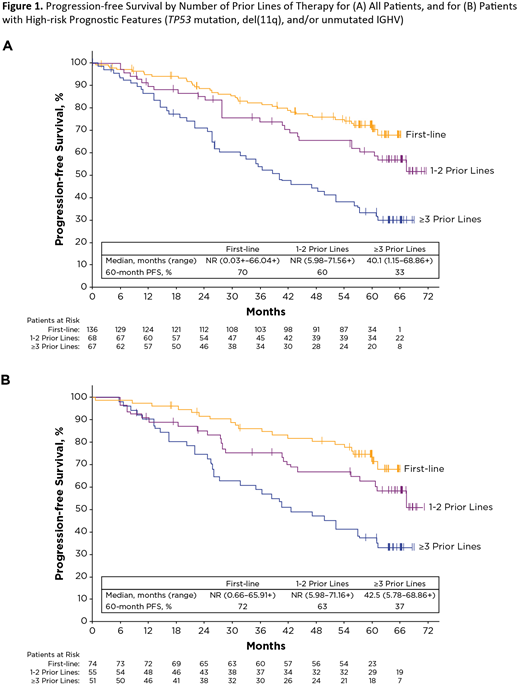
Results: This analysis of 271 patients included 136 patients in the first-line and 135 patients in the R/R groups (1-2 prior: n=68; ≥3 prior: n=67). Patients in the first-line group were older (median age [range], 73 years [65-89]) than those with 1-2 prior lines (65 years [30-86]) and ≥3 prior lines (67 years [44-83]). The proportion of patients with high-risk prognostic features was lower in the first-line group (first-line: 54%; 1-2 prior: 81%; ≥3 prior: 76%). Median follow-up was 59.8 months for first-line, 66.2 months for 1-2 prior, and 65.1 for ≥3 prior. Median PFS was not reached (NR) for first-line or 1-2 prior lines and was 40.1 months for ≥3 prior lines (Figure 1A). A greater proportion of patients treated with ibrutinib in earlier lines remained progression-free or alive at 60 months (first-line: 70%; 1-2 prior: 60%; ≥3 prior: 33%). First-line treatment resulted in a 34% reduction in risk of disease progression or death compared to 1-2 prior lines (HR: 0.66 [95% CI, 0.40-1.09]). PFS was significantly prolonged for first-line vs ≥3 prior lines (HR: 0.32 [95% CI, 0.21-0.49]) and 1-2 prior vs ≥3 prior lines (HR: 0.48 [95% CI, 0.30-0.77]). For patients with high-risk prognostic features, median PFS was NR for first-line or 1-2 prior lines and was 42.5 months for ≥3 prior lines (Figure 1B); treatment in earlier lines resulted in better PFS for these patients (first-line vs 1-2 prior, HR: 0.64 [95% CI, 0.35-1.18]; first-line vs ≥3 prior, HR: 0.33 [95% CI, 0.19-0.57]; 1-2 prior vs ≥3 prior HR: 0.51 [95% CI, 0.30-0.87]). Median OS for the overall population was NR (range, 0.10+-66.04+) for first-line, NR (5.98-71.56+) for 1-2 prior, and 67.4 months (1.15-69.78+) for ≥3 prior lines. The ORR was 91%, 94%, and 82% for first-line, 1-2 prior, and ≥3 prior lines, respectively. The CR rate (CR+CR with incomplete marrow recovery) was highest for the first-line group (first-line: 30%; 1-2 prior: 12%; ≥3 prior: 10%). At the time of analysis, 58% of patients remain on ibrutinib treatment in the first-line group. Prior to study closure, 38% of patients with 1-2 prior and 18% of patients with ≥3 prior lines remained on ibrutinib treatment. In the overall population, 8 patients (6%) in the first-line group discontinued due to progressive disease while it was the most common reason for discontinuation for patients with 1-2 (n=15, 22%) and ≥3 prior lines (n=25, 37%). Across all three groups, 52 patients (19%) discontinued due to adverse events (AEs) (first-line: n=29, 21%; 1-2 prior: n=13, 19%; ≥3 prior: n=10, 15%). AEs leading to dose reduction occurred in 20% of first-line, 13% of 1-2 prior, and 22% of ≥3 prior lines.
Conclusions: Overall, this integrated analysis of data with up to 6 years of long-term follow-up demonstrates that using single-agent ibrutinib in earlier lines of treatment results in better PFS, OS, and ORR with sustained efficacy for patients with CLL, including patients with high-risk prognostic features. During this extended follow-up, only 6% of patients treated in the first-line setting discontinued due to progressive disease. Ibrutinib was well tolerated with only 19% of patients across all lines of therapy discontinuing due to AEs.
Barr:Gilead: Consultancy; Verastem: Consultancy; Seattle Genetics: Consultancy; AbbVie: Consultancy; Pharmacyclics LLC, an AbbVie company: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding; Celgene: Consultancy; Merck: Consultancy; Genentech: Consultancy; Janssen: Consultancy; Astra Zeneca: Consultancy, Research Funding. Tedeschi:Janssen spa: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead: Consultancy; AbbVie: Consultancy, Membership on an entity's Board of Directors or advisory committees; SUNESIS: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; BeiGene: Honoraria; AstraZeneca: Membership on an entity's Board of Directors or advisory committees. Munir:AbbVie: Honoraria; Alexion: Honoraria; Gilead: Honoraria; Janssen: Honoraria; Novartis: Honoraria; Roche: Honoraria; Morphosys: Consultancy, Membership on an entity's Board of Directors or advisory committees; Sunesis: Consultancy; Pharmacyclics: Other: TBC; Acerta: Membership on an entity's Board of Directors or advisory committees. Hillmen:Acerta: Membership on an entity's Board of Directors or advisory committees; Apellis: Research Funding; Gilead: Research Funding; Roche: Research Funding; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy, Honoraria, Research Funding. Woyach:Janssen: Consultancy, Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy, Research Funding; AbbVie: Research Funding; Karyopharm: Research Funding; Loxo: Research Funding; Morphosys: Research Funding; Verastem: Research Funding. Byrd:Janssen: Consultancy, Other: Travel Expenses, Research Funding, Speakers Bureau; Pharmacyclics LLC, an AbbVie Company: Other: Travel Expenses, Research Funding, Speakers Bureau; TG Therapeutics: Other: Travel Expenses, Research Funding, Speakers Bureau; Novartis: Other: Travel Expenses, Speakers Bureau; Acerta: Research Funding; TG Therapeutics: Other: Travel Expenses, Research Funding, Speakers Bureau; Gilead: Other: Travel Expenses, Research Funding, Speakers Bureau; Ohio State University: Patents & Royalties: OSU-2S; Ohio State University: Patents & Royalties: OSU-2S; Genentech: Research Funding; Pharmacyclics LLC, an AbbVie Company: Other: Travel Expenses, Research Funding, Speakers Bureau; Acerta: Research Funding; Genentech: Research Funding; BeiGene: Research Funding. Ghia:ArQule: Consultancy, Honoraria; BeiGene: Consultancy, Honoraria; Juno/Celgene: Consultancy, Honoraria; Dynamo: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Acerta/AstraZeneca: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Research Funding; Sunesis: Consultancy, Honoraria, Research Funding; Novartis: Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy. Mulligan:AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Clinical Trial Participant, Research Funding, Speakers Bureau; GSK: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Clinical Trial Participant, Research Funding, Speakers Bureau; Roche: Consultancy, Honoraria, Other: Clinical Trial participant, Research Funding, Speakers Bureau; Commonwealth Serum Laboratories (CSL): Other: Clinical Trial participant; Sanofi-Aventis: Other: Clinical Trial participant; Acerta: Other: Clinical Trial participant. Dai:AbbVie: Equity Ownership; Celgene: Equity Ownership; Exelixis: Equity Ownership; Gilead: Equity Ownership; GSK: Equity Ownership; Pharmacyclics LLC, an AbbVie Company: Employment. Amaya-Chanaga:AbbVie: Equity Ownership; Pharmacyclics LLC, an AbbVie Company: Employment. Dean:AbbVie: Equity Ownership; Pharmacyclics LLC, an AbbVie Company: Employment. o'Brien:Pfizer: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy; Acerta: Research Funding; Alexion: Consultancy; Amgen: Consultancy; Aptose Biosciences, Inc: Consultancy; Astellas: Consultancy; Celgene: Consultancy; Eisai: Consultancy; Gilead: Consultancy, Research Funding; GlaxoSmithKline: Consultancy; Kite: Research Funding; Janssen: Consultancy; Pharmacyclics LLC, an AbbVie Company: Consultancy, Research Funding; Regeneron: Research Funding; Sunesis: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding; Vaniam Group LLC: Consultancy; Verastem: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal