

Background
B-cell receptor signaling inhibition (BCRi) is an effective treatment (trtmt) for patients (pts) with chronic lymphocytic leukemia (CLL), but resistance develops. Venetoclax selectively inhibits anti-apoptotic protein B-cell lymphoma 2 (BCL-2), and has demonstrated efficacy in relapsed/refractory CLL pts, particularly after BCRi. Venetoclax is started at 20 mg daily and escalated weekly over 5 weeks to the goal dose to avoid acute tumor lysis syndrome. However, we observed that many pts with relapsed/refractory CLL relapsing on BCRi progress more quickly than this schedule allows; they may progress while still taking BCRi or vigorously after its discontinuation. Given the need to promptly attain goal venetoclax dose in this population, we developed a rapid dose escalation scheme for venetoclax and reviewed our experience to understand the feasibility, safety, and efficacy of this approach in a properly equipped university setting.
Methods
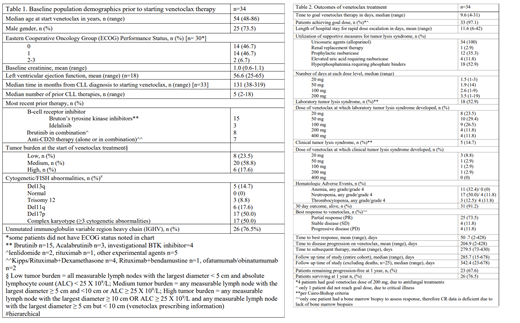
We retrospectively evaluated adult pts with relapsed/refractory CLL presenting to The Ohio State University who were treated with a "rapid dose escalation" of venetoclax. Charts were reviewed for previous and concomitant CLL treatments, tumor burden, prognostic factors, performance status, and co-morbidities. Venetoclax dosing was planned for a shorter time period than the 5 weeks described in the label dosing. The dose was increased as quickly as tolerated following the customary doses (20mg, 50mg, 100mg, 200mg, then 400mg). We reviewed the evaluated safety and efficacy outcomes with this approach.
Results
We treated 34 pts with rapid venetoclax dose escalation. Median age at venetoclax start was 54 years old and were 73.5% men. Pts had a median of 5 previous CLL trtmts (range 2-18). The most recent trtmt was single-agent BCRi in 18 cases, which overlapped with venetoclax in the majority. Only 6 pts had high tumor burden and the majority had low or medium tumor burden. Cytogenetic abnormalities at venetoclax start included: 17 (50.0%) pts with 17p deletion, 5 (14.7%) with 13q deletion, 6 (17.6%) with 11q deletion, and 3 (8.8%) with trisomy 12. Fifty percent of pts had a complex karyotype, and 76.5% had unmutated IGVH status. 24 (80%, n=30 pts that had testing done) pts had confirmed BTK/PLCу2 mutations. The mean time to goal venetoclax dose was 9.6 days (range 4-31); all but 1 pt reached goal dose. Eighteen (52.9%) pts developed tumor lysis syndrome (TLS) by lab criteria at doses from 20-400 mg, 5 pts developed TLS by clinical criteria, and 1 pt experienced grade 3 severity TLS (per Cairo-Bishop definition). Only 4 pts had an elevated uric acid requiring rasburicase. Seventy-three percent of pts achieved at least a partial remission, and 4 pts each had stable or progressive disease. Three pts died within 30 days: 1 from uncontrolled bleeding and neutropenia, 1 due to neutropenic sepsis with invasive fungal infection and gastric perforation, and 1 due to neutropenic septic shock and respiratory failure. Time to best response was mean 50.7 days (range 2-428). Median time to subsequent trtmt was 279.5 days (range 73-430). 23 pts (67.6%) had not progressed at 1 year, and 26 (76.5%) were surviving at 1 year.
Conclusion/summary
Rapid dose escalation of venetoclax in this pt population is safe and feasible. Despite a high percentage of patients developing TLS (52.9%), all patients recovered without lasting complications and all but one were able to achieve the goal dose of venetoclax. This dosing scheme achieved disease control with 67.6% remaining progression-free at 1 year and the majority of pts surviving. It is reasonable to implement venetoclax rapid dose escalation in the proper hospital setting with ample ancillary support. This approach may be needed for CLL patients with rapidly progressive disease on BCRi.
Dotson:Abbvie: Consultancy. Bhat:Pharmacyclics: Consultancy; Janssen: Consultancy. Byrd:Janssen: Consultancy, Other: Travel Expenses, Research Funding, Speakers Bureau; Gilead: Other: Travel Expenses, Research Funding, Speakers Bureau; Genentech: Research Funding; Ohio State University: Patents & Royalties: OSU-2S; Acerta: Research Funding; BeiGene: Research Funding; Pharmacyclics LLC, an AbbVie Company: Other: Travel Expenses, Research Funding, Speakers Bureau; Pharmacyclics LLC, an AbbVie Company: Other: Travel Expenses, Research Funding, Speakers Bureau; Janssen: Consultancy, Other: Travel Expenses, Research Funding, Speakers Bureau; Novartis: Other: Travel Expenses, Speakers Bureau; Genentech: Research Funding; Acerta: Research Funding; BeiGene: Research Funding; Ohio State University: Patents & Royalties: OSU-2S; TG Therapeutics: Other: Travel Expenses, Research Funding, Speakers Bureau; TG Therapeutics: Other: Travel Expenses, Research Funding, Speakers Bureau; Gilead: Other: Travel Expenses, Research Funding, Speakers Bureau; Novartis: Other: Travel Expenses, Speakers Bureau. Woyach:Janssen: Consultancy, Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy, Research Funding; AbbVie: Research Funding; Karyopharm: Research Funding; Loxo: Research Funding; Morphosys: Research Funding; Verastem: Research Funding. Awan:Genentech: Consultancy; Sunesis: Consultancy; Gilead: Consultancy; Abbvie: Consultancy, Speakers Bureau; Janssen: Consultancy; Pharmacyclics: Consultancy, Research Funding; AstraZeneca: Consultancy, Speakers Bureau. Rogers:AbbVie: Research Funding; Genentech: Research Funding; Janssen: Research Funding; Acerta Pharma: Consultancy.
Venetoclax- we will be suggesting a faster increase from starting to maximum/goal dose than the dosing label recommends. This is in order to achieve faster disease control.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal