

Introduction: Chronic Lymphocytic Leukemia (CLL) is a
clinically and biologically heterogeneous disorder that can be associated with immunological dysregulation. Several prognostic factors, such as IGHV status and chromosomal aberrations as trisomy 12, del11q, del13q or del17p have been detected so far. More recent genetic mutations, such as BIRC3, SF3B1, NOTCH1 and TP53 stratify even further the prognosis and the outcome in CLL patients (pts). However all data above reported, because of expensive techniques and experience typical of big laboratories, are not available to all medical centers. Therefore we considered necessary to identify more accessible and easy to perform parameters in all laboratories, as data concerning the presence of hypogammaglobulinemia, IgM or IgG monoclonal gammopathy, whose prevalence and impact on natural history of CLL in the medical literature are controversial, contradictory and not very significant because of few numbers in cohorts.
Therefore the first aim of the study was to evaluate the prevalence of monoclonal IgM/CLL, IgG/CLL and hypogammaglobulinemia compared with CLL pts with normal immunoglobulins (Ig) levels and to establish the impact on clinical outcomes based on Ig levels. The second aim was to find a correlation between each group of pts and biological data.
Methods: From four different Italian centers, we collected data from 1505 pts diagnosed with typical CLL from 1987 to 2017 and we divided them in four groups based on the presence of qualitative and quantitative alterations of serum immunoglobulins.
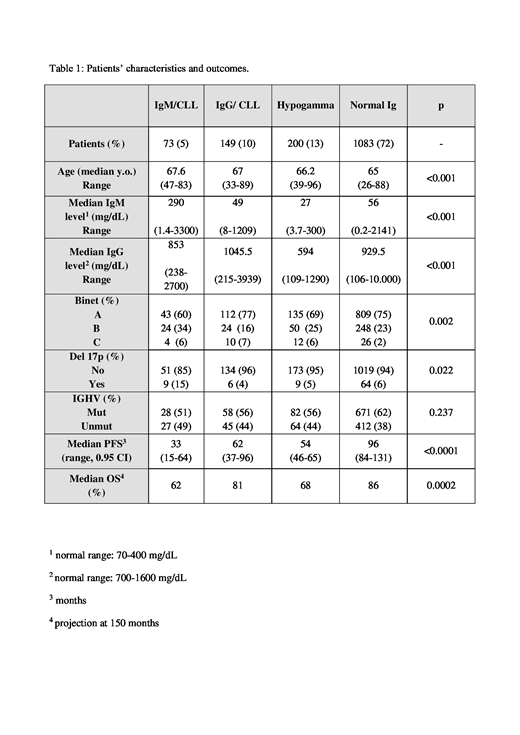
Baseline assessment and levels of serum Ig, immunofixation, chromosomal aberrations and clinical features were collected. [Table 1]. We evaluated the impact of each immunoglobulin subset on progression free survival (PFS) and overall survival (OS).
Results: Once assessment was made, we included in our study 1505 pts.
Median age of 65.5 was similar in all groups and data gathered from the four centers showed an overlapping rate about prevalence and time-dependent parameters in CLL pts and their related subclasses.
The overall prevalence of monoclonal gammopathy was 15%, of whom 149 pts (10%) with IgG/CLL and 73 pts (5%) with IgM/CLL. Hypogammaglobulinemia was detected in 200 pts (13%), while 1083 pts (72%) had no evidence of paraprotein or hypogammaglobulinemia.
The worst outcome group was identified among CLL with IgM paraprotein; moreover, this group of pts showed more advanced stages at diagnosis according to Binet staging (p<0.002) and a higher frequency of del17p with a percentage of 15% (p<0.022). [Table 1]. The worse median PFS observed was in IgM/CLL group, compared to Hypogamma/CLL, IgG/CLL, and normal/CLL: 33, 54, 62, 96 months respectively (p<0.0001). At the same time, a projection at 150-months showed an estimated OS of 62% in IgM/CLL group, versus 68% in hypogamma/CLL, 81% in IgG/CLL and 86% in normal/CLL (p<0.0001).
To evaluate if the specific deficit of IgG or IgM could have any unfavourable impact on each group's prognosis, we measured the serum levels of IgM and IgG in all pts. No statistically significant differences were observed among time-dependent parameters in IgG/CLL, IgM/CLL and hypogamma groups, based on IgM and IgG levels, if deficient or normal.Finally, in the group of pts who had normal gamma-level, median PFS and TTT was reached at 79 months (p=0.006 and 0.002, respectively) in the subgroup with IgM deficiency, while no statistical difference was observed regarding OS (p=0.785).
Conclusions: Our study provides data about prevalence and impact of monoclonal gammopathy and hypogammaglobulinemia on the outcomes of CLL patients. In this study, we observed that the 28% pts had any qualitative or quantitative immunoglobulins alteration, of whom 15% had monoclonal gammopathy and 13% had hypogammaglobulinemia. The worst outcomes were observed in the IgM/CLL pts in terms of PFS and OS. In conclusion, the laboratory data of serum Ig could be used as predictive markers of clinical outcomes because, for their easy availability, they could direct the prognosis of CLL pts. As a future perspective, we would like to characterize pts with monoclonal IgM component from a biological view, to correlate the subset of somatic mutations of the heavy chains of surface immunoglobulins with the monoclonal component and its prognostic significance.
Varettoni:ABBVIE: Other: travel expenses; Roche: Consultancy; Gilead: Other: travel expenses; Janssen: Consultancy. Trentin:ABBVIE: Honoraria, Other: board; Janssen: Consultancy, Honoraria, Other: Board; gilead: Consultancy; Roche: Honoraria, Other: Board.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal