

Introduction: Salvage immunochemotherapy (IC) followed by high-dose chemotherapy with autologous stem cell transplantation (autoSCT) is standard-of-care second-line therapy (2L) for patients with relapsed or refractory (R/R) diffuse large B cell lymphoma (DLBCL) deemed fit for autoSCT as per the CORAL study (J Clin Oncol. 2010 Sep 20;28(27):4184-90). Optimal therapeutic management of patients with R/R DLBCL who are autoSCT-ineligible is unknown. Here we describe the real-world outcomes of patients with R/R DLBCL who receive palliative intent 2L therapy in community and academic settings and do not receive autoSCT.
Methods: This analysis includes de-identified patients from the nationwide Flatiron Health electronic health record-derived database with a histologic diagnosis of DLBCL and R/R disease after frontline IC who do not undergo autoSCT and receive treatment with either bendamustine-based therapy, gemcitabine-based therapy, lenalidomide, or ibrutinib. Patients receiving rituximab/ifosfamide/carboplatin/etoposide (R-ICE) and high-dose cytarabine-containing second-line therapies were excluded. Event free survival (EFS) was defined as the interval between the start of current therapy and start of subsequent therapy if needed, last follow-up on current therapy, or death on therapy. Overall survival (OS) was defined as the time between start of current therapy and death or last follow-up while alive.
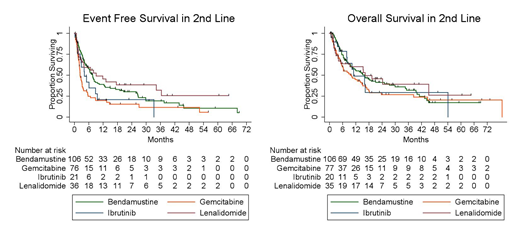
Results: A total of 250 patients were eligible for inclusion in 2L. Eight patients received autoSCT after gemcitabine therapy and were excluded from this analysis. Clinicopathologic characteristics at time of diagnosis include 56% male, 87% age >60, 55% ECOG performance status >1, 87% stage III-IV disease, 78% IPI >2, 56% germinal center (GCB) of those with cell of origin testing performed, 9% cMYC rearrangement positive when tested, and 29% transformed from indolent disease. A total of 106, 78, 36, and 22 patients received bendamustine, gemcitabine, lenalidomide, and ibrutinib, respectively. For all patients, median EFS was 5.1 months and median OS was 14.3 months in 2L. Median EFS was 7.6, 2.4, 9.1, and 4.2 months, and median OS was 16.0, 9.4, 16.3, and 11 months for bendamustine, gemcitabine, lenalidomide, and ibrutinib in 2L, respectively. Patients receiving bendamustine and lenalidomide demonstrated significantly improved EFS compared to those receiving gemcitabine (p=0.001 and 0.01, respectively), see Figure 1. We observed no difference in EFS (p=0.40) or OS (p=0.89) between lenalidomide and bendamustine in 2L. Univariate analysis demonstrated receipt of gemcitabine, ECOG PS>1, and IPI >2 to have statistically significant increased hazard for treatment failure and ECOG PS>1 to have an increased hazard for death in 2L relative to the reference group. Multivariate analysis demonstrated receipt of gemcitabine (HR 1.57, p=0.03 95% CI: 1.04 - 2.37) and ECOG PS>1 (HR 1.61, p=0.02 95% CI: 1.09-2.38) were associated with an increased hazard for treatment failure in 2L. Median EFS for patients on lenalidomide was 6.7 and 8 months (p=0.26), and median OS was 13.9 and 12.2 months (p =0.48) for patients with nonGCB and GCB cell of origin, respectively.
Conclusions: For patients with R/R DLBCL treated with palliative therapy in the 2L, bendamustine- and lenalidomide-based therapies resulted in significantly longer EFS compared to gemcitabine therapy. Although we cannot exclude the possibility that some patients received gemcitabine in 2L with the original intent to proceed with autoSCT, this does not contest our results as this therapy remains inferior to bendamustine and lenalidomide even if given to a potentially more fit patient population. Analysis shows no difference in outcomes by cell of origin if receiving lenalidomide in 2L. These findings may serve as benchmarks for outcomes following receipt of these therapies in the non-investigational setting and suggest both bendamustine and lenalidomide may be considered reasonable standard-of-care therapies for patients unfit for autoSCT in the 2L setting.
Landsburg:Celgene: Membership on an entity's Board of Directors or advisory committees; Triphase: Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Seattle Genetics: Speakers Bureau; Seattle Genetics: Speakers Bureau; Triphase: Research Funding; Takeda: Research Funding; Takeda: Research Funding.
Outcomes with lenalidomide and ibrutinib in patients with relapsed/refractory DLBCL will be discussed.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal