

Background: CHOP is widely used for untreated PTCL patients (pts), although it has limited efficacy. Chidamide is an oral benzamide class of HDAC inhibitor with subtype specificity in inhibition of HDAC 1, 2, 3 and 10, approved in China for relapsed or refractory PTCL at 30 mg twice per week. A Phase 1b/2 study (NCT02809573) is evaluating the safety, pharmacokinetics and preliminary efficacy of chidamide in combination with CHOP (CHOP-chidamide) in the first-line treatment for PTCL pts. Results from the study are reported.
Methods: This open-label, multicenter study enrolled pts (18~65 years) with previously untreated PTCL. Pts received one dose chidamide as the run-in treatment, and 4 days later the induction treatment of CHOP (6 cycles [each 21 days]) with chidamide on days 1, 4, 8 and 11. Pts who achieved a complete response or unconfirmed complete response (CR/CRu) at end of induction (EOI) received consolidation treatment with chidamide on days 1, 4, 8 and 11 every 21 days for 24 months maximum. A 3+3 design was employed in the chidamide dose-escalation stage with the starting dose at 20 mg. The first 21-day treatment cycle was a dose-limiting toxicities (DLTs) observation period (phase 1b; safety and pharmacokinetics), followed by a phase 2 cohort expansion stage. For pharmacokinetic (PK) evaluation, blood samples were collected at pre-dose and 1,2,4,8,12,24,48 and 72 h after the first dose of chidamide in the run-in period and in the first cycle of CHOP-chidamide. Primary endpoints were safety and tolerability of chidamide in combination with CHOP assessed by the incidence of adverse events (AEs) in both phase 1b and 2 and as DLTs during phase 1b. Secondary endpoint was efficacy as determined by the investigator.
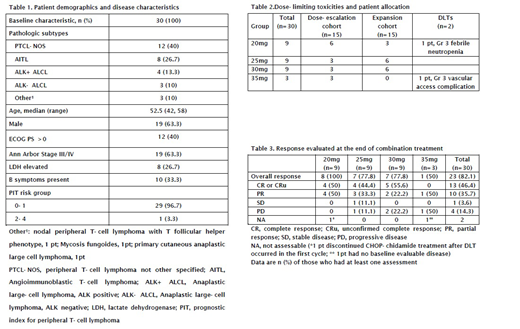
Results: Between Nov 15, 2016 and Aug 29, 2018, 30 pts were enrolled and received treatment. Pt demographics and disease characteristics are shown in Table 1. Fifteen pts were in the dose-escalation cohort and 15 in the expansion cohort (Table 2).One DLT with grade (Gr) 3 febrile neutropenia occurred in the first three enrolled pts in the 20 mg group, and 1 DLT with Gr 3 vascular access complication in the 35 mg group. Also, in the 35 mg group, 1 pt occurred Gr 2 neutropenia with sustained temperature >38℃, and the dose-escalation was stopped at this dose level. Serious AEs occurred in 7 (23.3%) of 30 pts during the combination treatment, including neutropenia (3 [10%]), leukopenia (2 [6.7%]), interstitial pneumonia (2 [6.7%]), thrombocytopenia (1 [3.3%]), febrile neutropenia (1 [3.3%]), pneumonia (1 [3.3%]), hyponatremia (1 [3.3%]), appendicitis (1 [3.3%]) and vascular access complication (1 [3.3%]). The most common (≥10%) Gr 3 or 4 treatment-related AEs were leukopenia (90%), neutropenia (83.3%), lymphocytopenia (40%), vomiting (13.3%), thrombocytopenia (10%) and febrile neutropenia (10%).No fatal AEs were reported. There were no apparently remarkable differences in frequency and intensity of AEs in pts between chidamide dose groups of 20 mg, 25 mg and 30 mg. Among 28 pts evaluable for response, 13 pts (46.4%) had a CR/CRu, 10 pts (35.7%) had a partial response, 1 pt (3.6%) had stable disease, and 4 pts (14.3%) had progressive disease (Table 3). Fifteen pts entered the consolidation phase (13 pts with CR/CRu, 1 pt with PR, 1 pt not evaluable), and the median treatment time was 189 days (35, 483). There was no AE leading to consolidation discontinuation. Progression-free survival (PFS) and overall survival (OS) at 12 months were 54.3% and 100%. At the data cutoff (Jan 8, 2019), median PFS was 14 months and median OS was not achieved. A total of 16 pts were evaluated in the PK analysis. Over the dose range from 20 to 35 mg, a linear and dose-dependent PK profile of chidamide was characterized in both monotherapy and combination treatment. In addition, co-administration of chidamide and CHOP did not significantly affect the plasma exposure of chidamide, with geometric mean ratio (combination vs monotherapy) values for Cmax and AUC were 97.6% (73.6%, 129.2%) and 97.9% (78.4%, 122.2%), respectively.
Conclusions: The combination of 20mg to 30 mg chidamide to a standard 3-week cycle of CHOP chemotherapy showed a manageable safety profile and favourable antitumour activity in pts with previously untreated PTCL. This combination could be further explored in comparison to CHOP alone in a randomized trial. CHOP-chidamide did not significantly alter the chidamide pharmacokinetics.
No relevant conflicts of interest to declare.
Chidamideis an oral benzamide class of HDAC inhibitor with subtype specificity in inhibition of HDAC1, 2, 3 and 10, approved in China for relapsed or refractory PTCL at 30 mg twice per week. This Phase 1b/2 study (NCT02809573) is evaluating the safety, pharmacokinetics and preliminary efficacy of chidamide in previously untreated PTCL patients.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal