

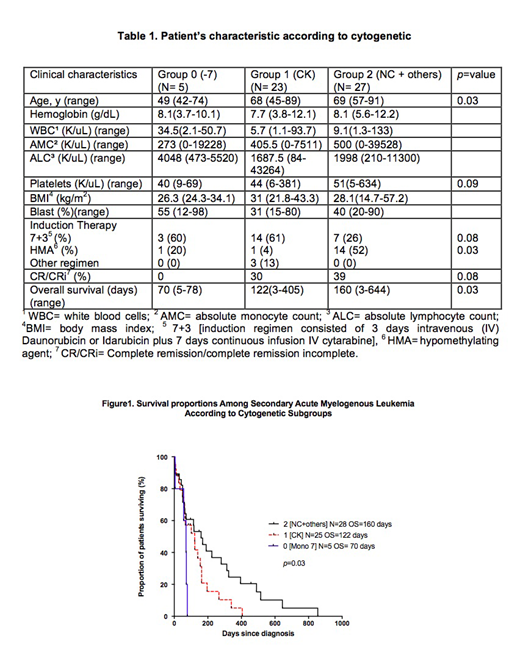
Background: Secondary acute myeloid leukemia (s-AML) [therapy-related (t-AML) and evolving from antecedent hematologic disorder, i.e. myelodysplastic syndrome (MDS), myeloproliferative neoplasm (MPN)] are highly aggressive disorders with 20% overall survival [OS] at 1 year. Challenges for initial therapy selection include 1. Difficulty for precise discrimination of pre-existing disorders [MDS vs MPN vs t-AML] and 2. Lack of reliable karyotypic/molecular risk stratification [i.e. European-leukemia-network-2017 [ELN 2017], originally designed for de novo AML]. In s-AML, enrichment for high-risk karyotypic and molecular abnormalities [i.e. complex karyotype (CK), -17p, -7/7p, p53, RUNX1, ASXL1 mutations] suggests that systematic stratification is feasible to adopt tailored therapy for complete remission [CR] success and OS estimation. In this study, our primary aim was to investigate clinical, cytogenetic and molecular predictors for CR and OS outcome among s-AML patient (pt). Methods: After IRB approval, 178 AML pt diagnosed in Baylor College of Medicine institutions [Michael E. DeBakey VA Houston and Baylor St. Luke's Medical Center] were screened. 68/178 [38%] s-AML pt were selected, however, 55/68(81%) had data available for analysis. Variables with known predictive value for AML prognosis were investigated including age, hemoglobin, white blood cell count [WBC], marrow blast percentage, pre-existing disease [MDS v MPN], karyotypic abnormalities and mutations obtained by next generation sequencing [NGS]. To identify cytogenetic subgroups with differential effect on survival, individual karyotypic abnormalities were "aggregated" into groups exhibiting similar OS [inferior v intermediate v superior survival, see Figure 1, group 0 v 1 v 2]. Kaplan Meier method was used to evaluate differential significant OS among cytogenetic groups. Linear regression model examined independent prognostic effect of "proposed cytogenetic stratification" when adjusting for potential confounders selected from our univariate analysis. Statistical analysis was performed with SAS software, NC, USA and Prism 5. Result: Median age of pt was 67 years (range 42-91). S-AML pt was Male 52/55 (96%), and white 36/55 (65%). Baseline characteristic for the 3 cytogenetic groups are depicted in Table 1. Median OS for all s-AML pt was 90.5 days [d] (range: 3-644). Pre-existing disease was available in 51/55 (93%) pt [10/51 (20%) MPN, 36/51 (70%) MDS, and 5/51(10%) t-AML (p=0.69)]. Intense [7+3] v less intense [hypomethylating agents (HMA)] therapy was delivered in 24/43 (56%), and 16/43 (37%), respectively. Karyotypic abnormalities were 5/55 (9%) monosomy 7, 23/55 (42%) CK [typical 14/23 (61%), and atypical 9/23 (39%)], and 27/55 (49%) abnormalities not classifiable as favorable or adverse (NC or <3 abnormalities not including -5q, -7q, and/or -17p). Median OS for group 0 [all -7] was 70 d (5-78). In intermediate cytogenetic, median OS was 122 d (3-405) [typical + atypical CK were aggregated in group 1 given equal OS (140 d vs 102 d, respectively, p= 0.3)]. Group 2 [NC +others] median OS was 160 d (3-644) [ANOVA, 0 v 1 v 2, p= 0.03] (Figure 1). Complete remission/complete remission incomplete [CR/CRi] rate was 0%, 30%, and 39% for 0 v 1 v 2 [0 v 1 p=0.1 and 0 v 2, p=0.08]. Importantly, in group 2, CR/CRi was 66% v 36%, in pt < and >60 y, respectively, p=0.05. Superior CR/CRi in pt <60 y was associated with absence of high-risk mutations [p53, ASLX1, RUNX1], p=0.008. Proposed cytogenetic stratification was the only independent predictor for survival among pt diagnosed with s-AML when controlled for all potential confounders (p= 0.015; 95% CI, 0.05-0.48). Conclusion: In s-AML with heterogeneous pre-existing disease and cytogenetic background, our "proposed cytogenetic stratification" retains ability to discriminate differential OS and odds for CR/CRi success. Our data adds "body of evidence" for selection of "differential" induction in s-AML cytogenetic subgroups predicted to have inferior CR/CRi and OS [i.e. HMA+ Venetoclax vs CPX 351 formulation, instead of standard 7+3]. It is conceivable that in pts with s-AML younger than 60 y who are assigned into cytogenetic subgroup 2 without high-risk mutations, 7+3 is reasonable induction while bridging toward allogeneic stem cell transplant.
Yellapragada:Novartis: Employment, Other: Spouse Employment ; Celgene: Research Funding; BMS: Research Funding; Takeda: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal