


Background: Allogeneic hematopoietic stem cell transplantation (HSCT) is currently the only potentially curative therapy in eligible patients with myelodysplastic syndromes (MDS). Reduced-intensity conditioning (RIC) regimens that have been developed to extend HSCT to older patients resulted in encouraging outcomes. However, several retrospective studies have raised concerns about disease control when RIC is used in MDS and the ideal conditioning regimen has not yet been found. In this study, we aimed to compare two most commonly used RIC regimens; intravenous use of fludarabine with busulfan (FluBu) and fludarabine with melphalan (FluMel).
Study population: Through the CIBMTR, after excluding patients with ex-vivo T cell depletion, we identified 1045 MDS patients aged ≥ 60 years and underwent first HSCT with matched related or matched (8/8) unrelated donor (MRD and MUD) using RIC between 2007-2016.
RIC was defined via CIBMTR criteria as a regimen that incorporated an IV busulfan (BU) total dose ≤ 7.2 mg/kg or low-dose melphalan (MEL) total dose ≤ 150 mg/m2. By that, we identified 697 MDS patients who received FluBu (BU 6.4 mg/kg: 87%, BU 3.2 mg/kg: 13%) and 448 receiving FluMel (MEL 140 mg/m2: 80%, MEL 100 mg/m2: 20%).
Results: The two groups, FluBu and FluMel, were comparable for disease and transplant related characteristics except the more frequent use of ATG or Campath in FluBu group (39% vs. 31%). The median age was 67 in both groups, and 26% and 19% of FluBu and FluMel groups were aged ³70, respectively. Hematopoietic comorbidity index (HCT-CI) was ³3 in 61% and 59% of FluBu and FluMel groups and MDS risk score by CIBMTR at HCT was high/very high in 34% in both groups.
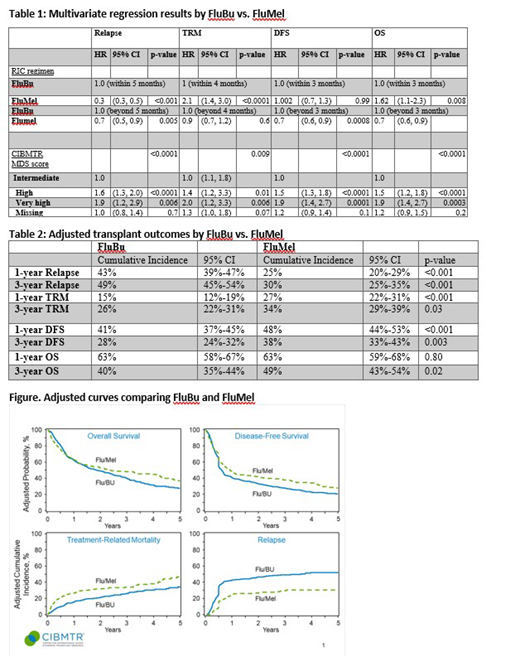
FluMel was associated with a reduced relapse incidence (RI) after HSCT compared with FluBu as presented in Table 1 and Table 2. Adjusted RI at 1-year was 43% with FluBu and 25% with FluMel (p=<0.0001). On the other hand, transplant related mortality (TRM) was higher with FluMel compared with FluBu (27% vs. 15%, p=<0.0001). The difference persisted at 2- and 3-years after HSCT as presented in the figure. Since the magnitude of improvement in RI was greater with FluMel than the improvement in TRM with FluBu, disease-free survival (DFS) was improved at 1-year and beyond with FluMel compared with FluBu (48% vs. 41% at 1-year, p=0.030, and 38% vs 28% at 3-years, p=0.0030). These outcome differences remained significant when sensitivity analyses were performed excluding patients who received RIC with either BU 3.2 mg/kg or Mel 100 mg/m2.
FluMel, did not lead to higher incidence of severe grade 3-4 aGvHD (HR=1.2, 95%CI, 0.9-1.6, p=0.3) or chronic GvHD (HR=0.9, 95%CI=0.7-1.06, p=0.2). However, grade 2-4 aGVHD was observed more often with FluMel than FluBu (HR=1.3, 95%CI, 1.1-1.6, p=0.006). This led to inferior outcomes of GRFS within the first 2 months with FluMel (HR=1.9, HR=1.4-2.6, p<0.001) but superior outcomes of GRFS beyond 2 months with FluMel compared with FluBu (HR=0.7, 95%CI=0.6-0.8, p<0.001).
Conclusion: Our results suggest that between the two most commonly used RIC regimens in older MDS patients, FluMel was associated with superior DFS and overall survival compared with FluBu due to reduced RI despite higher TRM.
Oran:AROG pharmaceuticals: Research Funding; Astex pharmaceuticals: Research Funding. Nakamura:Kirin Kyowa: Other: support for an academic seminar in a university in Japan; Alexion: Other: support to a lecture at a Japan Society of Transfusion/Cellular Therapy meeting ; Celgene: Other: support for an academic seminar in a university in Japan; Merck: Membership on an entity's Board of Directors or advisory committees. Scott:Celgene Corporation: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Alexion: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Research Funding; Incyte: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Agios: Speakers Bureau. Popat:Jazz: Consultancy; Incyte: Research Funding; Bayer: Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal