

Introduction: Venous thromboembolism (VTE) encompasses a spectrum of disorders involving thrombosis in the venous circulation, namely deep vein thrombosis (DVT) and pulmonary embolism (PE). The incidence of thrombosis is significantly elevated in patients with malignancy due to a hypercoagulable state. In addition to the elevated risk of thrombus formation in patients with malignancy, certain tumours have a predilection for intravascular extension, termed tumour thrombus. The presence of tumour thrombus considerably worsens prognosis, alters staging, and can influence the treatment options for these patients. While tumour thrombus can have have a significant impact on patients, the clinical course and optimal management of tumour thrombus remains unknown. We aim to describe the natural history of tumour thrombus and compare outcomes in those treated with or without anticoagulation at our centre.
Methods: We performed a retrospective, observational review of patients over 16 years of age with tumour thrombus at a single-centre between January 2008 and December 2017. Patients with documented tumour thrombus on computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound (US) were included in this study. Patients already on anticoagulation were excluded. Data were collected through medical record review including baseline characteristics, treatment history, complications and clinical outcomes. Overall survival and VTE recurrence rates between those treated with or without anticoagulation were demonstrated using Kaplan-Meier survival curves and Log-rank test. Cox-proportional hazards models were used to estimate the hazard ratio for tumor thrombosis with and without adjustment for patient characteristics including comorbidities, treatment, acuity, and location.
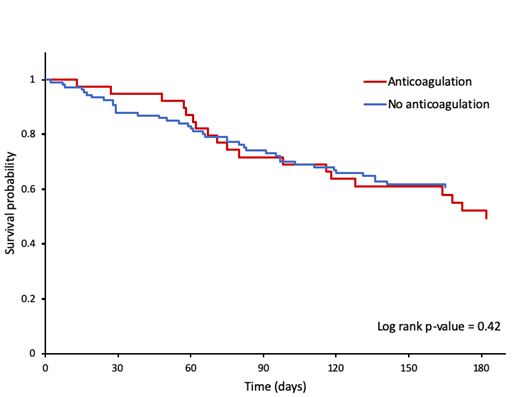
Results: A total of 153 patients were identified to meet inclusion criteria over the study period. The majority of patients were male (65.4%) with an mean age of 65.7. The most common malignancies associated with tumour thrombus were renal cell carcinoma (34.6%) and hepatocellular carcinoma (28.8%), with 125 patients (82.5%) having stage III or IV malignancies. The most common locations of tumour thrombus were the portal vein (37.5%), renal vein (32.9%) and inferior vena cava (26.3%). Forty-one patients (26.8%) were treated with anticoagulation. Of the entire study population, 18 patients (11.8%) developed VTE within a 6 month study period after being diagnosed with tumour thrombus. Of those that developed VTE following a diagnosis of tumour thrombus, 11 were on anticoagulation (61%) and 7 were not (39%). Five patients receiving anticoagulation experienced major bleeding. Mortality was 42.5% at 6 months with no significant difference in survival between those treated with or without anticoagulation (Figure 1; p = 0.42). Proportion hazards models were not completed at the abstract submission deadline; full study results will be presented at the ASH meeting.
Conclusion: In our study, we show that there is no significant difference in survival between patients with tumour thrombus treated with or without anticoagulation. While there is no clear evidence that anticoagulation improves outcomes across all patients with tumour thrombus, further studies are needed to identify subgroups of patients who may benefit from anticoagulation given their increased risk of VTE.
Keating:Sanofi: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria; Seattle Genetics: Consultancy; Janssen: Membership on an entity's Board of Directors or advisory committees; Shire: Membership on an entity's Board of Directors or advisory committees; Hoffman La Roche: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal