

Introduction
Cancer and its treatments are well-recognized risk factors for the development of venous thromboembolism (VTE). However, the risk of developing VTE varies greatly among individuals, depends on several factors. Yet, the commonly used prediction models for cancer-associated thrombosis (CAT) mostly focus only on patients with solid cancers treated in an ambulatory setting. Their applicability in patients with hematologic malignancies or inpatient cancer cares is limited.
Here we aimed to develop and validate a simple clinical prediction model for CAT in newly diagnosed hematologic malignancies and solid cancers patients treated with chemotherapy, to be used both in an ambulatory and inpatient setting to enhance its generalizability.
Methods
Data of consecutive patients, 18 years of age or older, with a newly diagnosis of both hematologic malignancies or solid cancers who were diagnosed and treated with chemotherapy at our institution between 2008 to 2015 were included in this analysis. Patients without a histologically confirmed cancer diagnosis or those who were treated with anticoagulantion were excluded. Patients were followed up from date of cancer diagnosis until VTE occurrence, death, or censoring at 36 months.
The primary outcome was cumulative incidence (CI) of objectively confirmed VTE at 6 months after cancer diagnosis.
To develop the CAT-CR model, a Fine and Gray competing risk regression with stepwise selection was used to select prognostic variables included in the model, treating death not related to VTE as a competing event. Variables with P value < 0.05 were included in the final model.
A risk score was then calculated from the sum of adjusted β regression coefficient weighted points from all significant risk factors for each patient.
The internal validation was done using bootstrap resampling method to generate new 1,000 datasets by random sampling of the original data with replacement. Multivariable competing risk regression with the same condition as in the original data set was then calculated for the new data sets in order to obtain the bootstrap parameter estimates. Harrell's C-concordance index and area under time-dependent receiver operating characteristic curves (AUC) associated with risk of VTE within 6 months were used to assess the discrimination ability of the model.
Results
A total 1598 patients were included in the analysis with a median age of 59 years (range 18-94). Primary sites of cancer were breast (N=344, 21.5%), colon (N=262, 16.4%), gynecologic (N=174, 10.9%), hematologic malignancies (N=335, 21%) and others (N=483, 30.2%) while 1070 patients (67%) were in advance stage disease. Khorana risk score were low, intermediate and high in 597 (37.4%), 882 (55.2%) and 119 (7.5%) patients, respectively. VTE was developed in 86 patients (5.4%) with cumulative incidence at 6 months of 2.33%.
Factors associated with a significantly increased risk of VTE included in the final model were age > 60 years, advance stage, high risk cancer (gynecologic, lung, stomach, pancreas, esophagus, liver), ECOG performance status 3-4, inpatient chemotherapy, and hemoglobin < 10 g/dl. with score weighted assignment of 1, 1, 2, 2, 2 and 2, respectively.
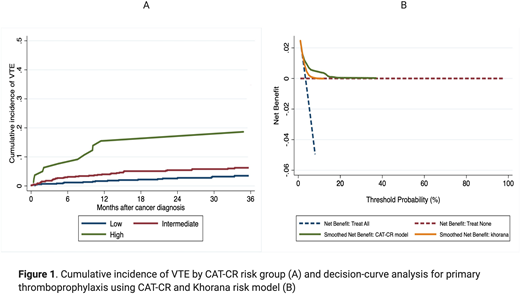
Patients were then divided into 3 CAT-CR risk groups: low (score 0-3, N=714), intermediate (score 4-5, N=803) and high (score > 5, N=81) with the CI of VTE at 6 months of 1.01%, 2.98% and 7.66%, respectively (P<0.001) (Figure 1A).
Compared with low risk group patients in intermediate and high risk group had a significantly increased risk of VTE with the subdistribution hazard ratio (SHR) of 1.68 (1.24-2.71, P0.032) and 5.15 (2.59-7.22, P<0.001) in the developing cohort and 1.74 (1.28-2.93, P0.022) and 2.96 (2.37-6.53, P<0.001) in bootstrap validation datasets.
The CAT-CR model had good discrimination ability with C-index of 0.681 and AUC of 0.773. The decision-curve analysis showed that the model had greater clinical utility for thromboprophylaxis indication than did the strategies of treat all or treat none and better than the commonly used Khorana risk model. (Figure 1B)
Conclusions
The CAT-CR model can be successfully used to predict the occurrence of VTE in patients with hematologic malignancies and solid cancers who are treated in both ambulatory and inpatient setting. The improved generalizability of the CAT-CR model could aid physicians in selection of high risk cancer patients who will most benefit from thromboprophylaxis.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal