

Background: Hemophagocytic lymphohistiocytosis (HLH) can be life-threatening if not detected and treated appropriately. Diagnosing HLH can be confusing due to other similar febrile diseases that present with cytopenia. Although a decrease in natural-killer cell (NK)-cytotoxicity is an important diagnostic parameter for primary HLH, the role in adult HLH has not been well-defined.
Aim: To identify the diagnostic relevance and the significant cut-off values for NK cytotoxic function, we focused on patients that presented with fever with either cytopenia or evidence of hemophagocytosis. NK cytotoxicity was calculated at the time of diagnosis and we tried to identify significant differences between the causes of disease. Finally, the overall treatment response and survival outcomes were also evaluated based on the level of NK cytotoxicity in several subgroup analyses.
Methods: We prospectively enrolled 123 adult patients that presented with fever accompanied by either cytopenia in at least two lineages or marrow hemophagocytosis. A diagnosis of HLH was based on HLH-2004 criteria and treated based on HLH-94 protocol. HLH-suspected patients were initially treated with 10mg/BSA of dexamethasone, and etoposide was considered if clinical improvement was not observed within 7 days after dexamethasone. Patients other than HLH were treated with disease-specified therapy. NK-cytotoxicity was calculated at diagnosis by K562-cell direct lysis using flow-cytometry.
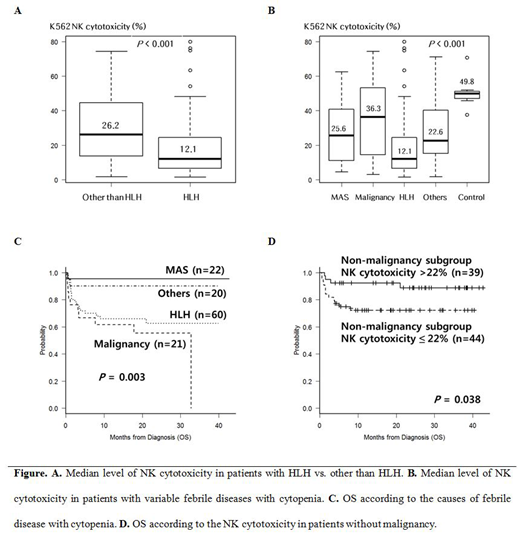
Results: HLH (n=60) was determined to be caused by Epstein-Barr virus (EBV, n=11), infection other than EBV (n=16), malignancies (n=19), and unknown (n=14). Febrile diseases other than HLH (n=63) were diagnosed as rheumatologic disease (n=22), malignancies (n=21), infection (n=12), non-malignant hematological diseases (n=6), and unknown (n=2). The results revealed that an HLH diagnosis was significantly correlated with lower NK-cytotoxicity, compared to other diseases (12.1% vs. 26.2%, p<0.001), and a value less than 22% was a relevant cut-off for diagnosing HLH. Additionally, lower NK-cytotoxicity showed inferior 2-year overall survival in the non-malignancy subgroup (72.2% vs. 88.8%, p=0.038). Multivariate analysis showed that low NK-cytotoxicity, splenomegaly, and marrow hemophagocytosis were independent diagnostic parameters for HLH, and low NK-cytotoxicity and EBV-association were related with poor survival outcomes in non-malignant febrile diseases.
Conclusion: We determined that decreased NK-cytotoxicity is a relevant marker that can be used for diagnosis of adult HLH compared with several similar febrile diseases and is also related to poor OS in non-malignant febrile diseases. Based on these results and other prospective studies, we hope that additional relevant diagnostic criteria for adult HLH can be identified in the near future.
Kim:Celgene: Consultancy, Honoraria; Astellas: Consultancy, Honoraria; Hanmi: Consultancy, Honoraria; AGP: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; SL VaxiGen: Consultancy, Honoraria; Novartis: Consultancy; Amgen: Honoraria; Chugai: Honoraria; Yuhan: Honoraria; Sanofi-Genzyme: Honoraria, Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Handok: Honoraria; Janssen: Honoraria; Daiichi Sankyo: Honoraria, Membership on an entity's Board of Directors or advisory committees; Otsuka: Honoraria; BL & H: Research Funding. Lee:Alexion: Consultancy, Honoraria, Research Funding; Achillion: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal