

Background: Vitamin D, in addition to its role in calcium and bone homeostasis, is a multifunctional regulator of inflammation and of innate and adaptive immune responses. Deficiencies are prevalent in sickle cell disease. We conducted a randomized double- blind active-controlled clinical trial comparing high- (100,000 IU/month) and low-dose (12,000 IU/month) oral vitamin D3 in 62 children with sickle cell disease to reduce respiratory complications including infection, asthma exacerbation and acute chest syndrome (ViDAS trial: Vitamin D for sickle cell respiratory complications; NCT01443728). A secondary aim was to examine the effects of vitamin D on immune function and inflammation.
Methods: Using stored serum samples collected from subjects at steady state, we examined hsCRP (single-plex assay) and key cytokines and markers of vascular activation (20-plex immunoassay) at baseline and year-1 in a subset of 36 subjects with HbSS (high-dose: n=17; low-dose: n=19), mean age 7.8 years, 53% females and 67% on hydroxyurea. Immune markers included IL1β, IL1RA, IL2, IL4, IL10, IL18, IL22, IFNγ, TNFα, TNFβ, sFasL, CXCL1, CXCL8 (IL8), PDGFBB, VEGFA, serpin E1 (PAI1), sICAM1, VCAM1, TGFα and TGFβ. Raw immune data were transformed using Box-Cox transformations and standardized; markers with persistently skewed (non-Gaussian) distributions after transformation were dichotomized for analysis. Continuous immune variables were analyzed by repeated measures ANOVA (unadjusted) and ANCOVA (adjusted for baseline covariates of age, sex and baseline total 25-hydroxyvitamin D3 and D2). Dichotomized biomarkers were analyzed using generalized linear mixed-effects models. Secondary analyses stratified on hydroxyurea status were also pursued. For these exploratory biomarker discovery-focused analyses, all significance tests were performed 2-tailed without adjustment for multiple comparisons, with α=0.1 for main effects and 0.2 for interactions.
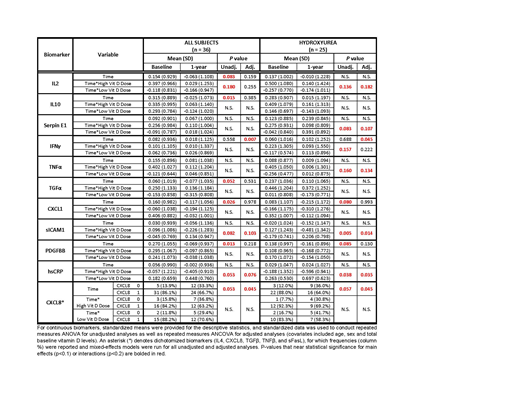
Results: Independent of vitamin D3 dose, serum concentrations of immune markers declined from baseline to the 1-year timepoint for the pro-inflammatory markers IL2, CXCL8 (IL8), IFNγ, TGFα, CXCL1 and PDGFBB and the counter-regulatory molecule, IL10. Among all subjects, interactions of dose group*time were found for IL2, sICAM1 and hsCRP; subjects on hydroxyurea additionally demonstrated dose group*time interactions for serpin E1 (PAI1), IFNγ and TNFα. Subjects on hydroxyurea in the high-dose group also demonstrated decreases over 1-year follow-up in serum IL2, serpin E1, IFNγ, TNFα, sICAM1 and hsCRP whereas serum levels of these immune markers increased among subjects in the low-dose group taking hydroxyurea. This crossover pattern in direction of the dose group*time interaction effect was also observed for the larger study population for sICAM1 and hsCRP. Table 1 shows the markers that tested significantly for main effects and/or interactions. Effects for the rest of the markers were not statistically significant.
Conclusions: Our data support the immunomodulatory properties of vitamin D, with variable responses to high and low doses. Effects involved several salient immune and vascular markers for sickle cell disease, including IL2, serpin E1, IFNγ, TNFα, sICAM1 and hsCRP, and appeared to be more pronounced among subjects on high-dose vitamin D3 who were also taking hydroxyurea.
Brittenham:Nestec, Inc.: Consultancy; Novartis International: Consultancy; Tesseract Health, Inc.: Consultancy; Vifor Fresenius Medical Care: Consultancy; Ambys Medicines: Consultancy; Dispersol Technologies: Consultancy; Rockwell Medical, Inc.: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal