

Introduction: Millions are affected by Sickle Cell Disease (SCD) worldwide with the greatest burden in sub-saharan Africa. Its origin thought to lie within the malaria belt of the world, SCD continues to affect thousands of lives worldwide partly due to the migration patterns of the human race to different continents. We created the Consortium for the Advancement of Sickle Cell Research (CASiRe) to better understand the different phenotypes of SCD and compare the clinical profiles of patients living in different environments through a validated questionnaire and medical chart review, standardized across 4 countries (United States[U.S.] United Kingdom[U.K.], Italy and Ghana). For this report, we recorded the multi-generational ethnic and racial background of 877 SCD patients across the CASIRE cohort for our final analysis.
Methods: CASiRe included 6 sites in the U.S. (Univ. of Michigan, Rainbow Babies & Children's Hospital, Promedica Toledo Children's Hospital, Children's Hospital at Montefiore, Connecticut Children's Medical Center, Univ.of Connecticut Health Center), 2 in Ghana(Ghana Institute of Clinical Genetics, Pediatric SCD Clinic at Korle Bu Teaching Hospital), 2 in Italy( Univ. of Campania Luigi Vanvitelli, Univ. of Padua, Italy), and U.K.(Guys & St. Thomas Hospital, Evelina Children's Hosp). Between 2011 and 2017, after obtaining IRB approval at each site and written informed consent, demographic, clinical and laboratory data were collected by interviewing the patient and/or parent/guardian At the 2 sites (Guys and St Thomas Hospital, UK; Univ. of Padua, Italy) with existing IRB approved SCD registries data were abstracted directly from their respective databases. Descriptive statistics were performed on a subset of demographic data that included: age, race, gender, sickle cell genotype, country of birth of patient, parents, and grandparents. The geographic region and country of origin was based on parents' country of birth and separated into 10 regions: W.Africa, C.Africa, N Africa, Caribbean, C. America, N America, Europe, S America, Asia, Middle East.
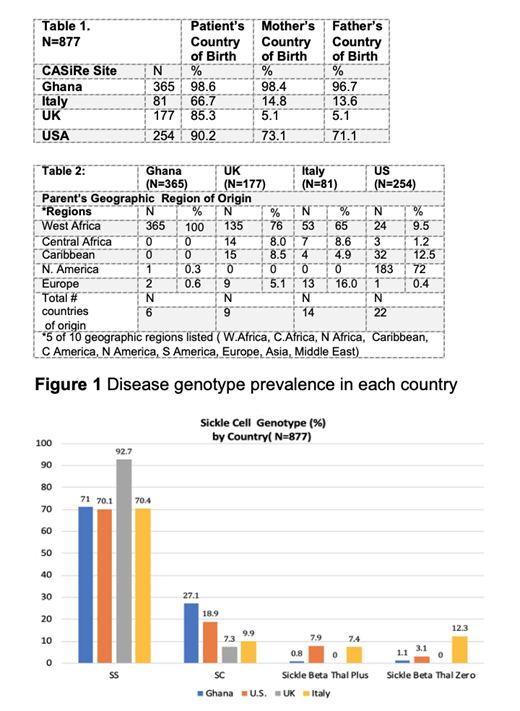
Results: 877 patients were enrolled with a median age 19.3 years. 451 (51.4%) patients were children, 424 (48.3%) male. Ghanaians represented 41.6% (365) of patients, while 254 patients (29%) were from the U.S. Italy enrolled 81 patients (9.2%), and 177 patients (20.2%) were from the U.K. West Africa represented the largest geographic region of origin of(577/65.8%), followed by N. America (184/21%), Caribbean (51/5.8%), Europe (27/3.1%), and Central Africa (24/2.7%). Overall(Fig. 1), 75% of patients (658) had Hgb SS, 168 patients (19.2%) had Sickle C disease, 29 (3.3%) had Sβ+thal and 22 patients (2.5%) of patients had Sβ0 thal. Racially, 820 patients (93.5%) identified themselves as African American or Black, while 30 patients (3.4%) identified themselves as Caucasian and 21 patients (2.4%) identified themselves as Latino or Hispanic. All Ghanaians identified as Black, while in the US and UK, over 90% of patients identified themselves as Black, and about 3% reported themselves as Caucasian. In comparison, in Italy, over 76% of patients reported a Black racial background, while 21% reported Caucasian background. (Table 1 and 2)>98%Ghanaian patients and their parents were born in Ghana. In contrast, 66.7% of patients and <15% of parents in Italian sites were born in Italy with the 64% of parents emanating from West Africa (38% Nigeria).Over 85% of patients in the UK were born in the UK while only 5.1% of parents were born there (54% in Nigeria). In the US, >90% of patients were born within the US; Parents of patients were born in America 70% of the time. Caribbean (12.5%) and West African countries(9.5%) were the next highest parent countries of origin. 32 different countries of origin were reported within our cohort with the US leading with 22 different countries.
Conclusion: This study is the first to describe the geographic distribution of these migrations in a very large cohort of nearly 900 patients with SCD.West Africa represented the largest geographic region of origin for SCD patients in Europe while Caribbean was the leading Non-US geographic region of origin in American patients. The diverse ethnic backgrounds observed in our cohort raises the possibility of how genetic and environmental heterogeneity within each SCD population subgroup can have implications on the clinical phenotype and clinical research outcomes.
Campbell:Novartis: Research Funding; Cyclerion: Consultancy, Research Funding; Global Blood Therapeutics: Consultancy, Research Funding. Colombatti:Novartis: Consultancy; Global Blood Therapeutics: Consultancy; AddMedica: Consultancy. Andemariam:NovoNordisk: Membership on an entity's Board of Directors or advisory committees; New Health Sciences: Membership on an entity's Board of Directors or advisory committees; Global Blood Therapeutics: Other: DSMB Member; Bluebird Bio: Membership on an entity's Board of Directors or advisory committees; Emmaus: Membership on an entity's Board of Directors or advisory committees; Cyclerion: Membership on an entity's Board of Directors or advisory committees; Imara: Research Funding; Sanofi Genzyme: Membership on an entity's Board of Directors or advisory committees; Community Health Network of Connecticut: Consultancy; Terumo BCT: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Strunk:Novartis: Membership on an entity's Board of Directors or advisory committees; Global Blood Therapeutics: Speakers Bureau. Piccone:Hemex Health, Inc.: Patents & Royalties. Manwani:GBT: Consultancy, Research Funding; Novartis: Consultancy; Pfizer: Consultancy. Perrotta:Novartis: Honoraria, Research Funding; Acceleron Pharma: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal