

Background: Hydroxyurea (HU) is an imperative disease-modifying agent in the treatment of sickle cell anemia (SCA). Over the past 30 years, numerous clinical trials have demonstrated both safety and efficacy of this medication in prevention of acute and long-term complications of SCA; however HU continues to be under-utilized in clinical practice. Possible reasons include a lack of provider and family education on the drug, a family's belief in the lack of severity of their child's disease, families not wanting to add additional medications to daily routine and fear of side effects. We sought to increase HU use by a multi-pronged approach of using provider and family education, information technology (IT) tools and weekly reinforcement at pre-visit planning (PVP) team meetings.
Methods: We conducted provider education sessions to disseminate knowledge about HU. These included review of NHLBI guidelines, dosing guidelines and tips to optimize HU use and merits of escalating to maximum tolerated dose. The target audience was physicians, fellows, mid-level providers and nurses. ECHO sessions provided by a regional collaborative augmented this effort. A consensus HU guideline document was readily available electronically.
The IT team in collaboration with the sickle cell team modified the clinic visit electronic note. The new note included check boxes to document eligibility for HU (based on sickle cell phenotype and severity of disease), and initial and ongoing HU counselling. A table in the clinic note tracked HU dose modifications. A practical algorithm regarding initiation, escalation and monitoring of HU was available as a pop-up in the note to assist providers. An electronic "Sickle Cell Dashboard" was created using real-time data. The dashboard flagged HU eligible patients not yet started on HU. Strategies to successfully initiate HU therapy for these patients were discussed at weekly PVP meetings. We provided HU counselling early and often during first months of life. Successful counselling strategies were shared among providers at PVP meetings. Ancillary staff was trained in utilization of dashboard.
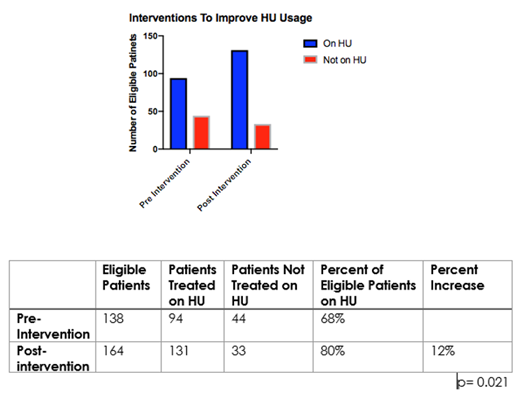
Percentage of HU eligible patients who were prescribed HU was measured for two periods: August 1, 2017 to July 31, 2018 (pre-intervention) and August 1, 2018 to July 31, 2019 (post-intervention). A two-sided Fisher's exact test measured statistical significance.
Results: In the pre-intervention period 94 of 138 (68%) HU eligible patients were prescribed HU. In the post-intervention period 131 of 164 (80%) HU eligible patients received HU prescription. The 12% increase was statistically significant (p=0.021). Increased education and counselling fostered provider enthusiasm and confidence in prescribing HU. An early start of HU therapy resulted in better compliance with treatment. The collaboration with IT team and creation of electronic "Sickle Cell Dashboard" identified several areas of improvement and inspired additional quality improvement projects.
Discussion: Aggressive provider and family education, enhanced electronic records, weekly PVP meetings, readily available HU dosing guidelines and an automated dashboard to flag eligible patients for targeted counselling improved the utilization of this important disease-modifying agent in a significant way. Further improvements can be made by monitoring pharmacy database for prescription fill rates, flagging patients who are overdue for follow-up visits and providing ongoing counselling. Infrastructure established for and lessons learned from this project can be applied to improve comprehensive care for SCA in a sustainable and cost-effective fashion.
Gomez:Alnylam: Consultancy; Novo Nordisk, Novartis, Pfizer, Sanofi, Takeda, UniQure: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal